Das könnte Ihnen auch gefallen
- Fluid & ElectrolyteDokument26 SeitenFluid & Electrolytesanjana bhatia100% (1)
- Cardiogenic ShockDokument20 SeitenCardiogenic Shockanimesh pandaNoch keine Bewertungen
- First Aid - CPR - AED Participant's ManualDokument196 SeitenFirst Aid - CPR - AED Participant's Manualadamiam100% (2)
- Vasoactive DrugsDokument61 SeitenVasoactive DrugsAde Gustina SiahaanNoch keine Bewertungen
- Sample Personal Statement For FellowshipDokument1 SeiteSample Personal Statement For FellowshipAbdul Basit Saeed100% (11)
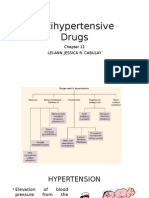
- Antihypertensive DrugsDokument37 SeitenAntihypertensive Drugsleiann_jessicaNoch keine Bewertungen
- HypertensionDokument85 SeitenHypertensionmelkamu AssefaNoch keine Bewertungen
- Drugs Acting in CVSDokument63 SeitenDrugs Acting in CVSMeghan Norico Cristuta100% (1)
- Management of Shock: Role of Inotropic & Vasoactive DrugsDokument50 SeitenManagement of Shock: Role of Inotropic & Vasoactive DrugsbajaocNoch keine Bewertungen
- Vasoactive TherapyDokument26 SeitenVasoactive Therapylidya agustin100% (1)
- Remedial Part 2Dokument13 SeitenRemedial Part 2Prince Rener Velasco PeraNoch keine Bewertungen
- Shock: Erdiansyah Zulyadaini, MD, FIHA FK Universitas Muhammadiyah Purwokerto/ RSUD Dr. Soeselo Kabupaten TegalDokument47 SeitenShock: Erdiansyah Zulyadaini, MD, FIHA FK Universitas Muhammadiyah Purwokerto/ RSUD Dr. Soeselo Kabupaten TegalFarah AkhwanisNoch keine Bewertungen
- Drugs Affecting The Cardiovascular SystemDokument70 SeitenDrugs Affecting The Cardiovascular SystemRayne Bonifacio100% (2)
- Practice Questions - EDNDokument6 SeitenPractice Questions - EDNKaren BlancoNoch keine Bewertungen
- Letters Combined (11 Referral, 2 Discharge, 1 Transfer)Dokument49 SeitenLetters Combined (11 Referral, 2 Discharge, 1 Transfer)Faisal ImtiazNoch keine Bewertungen
- Fccs - ShockDokument27 SeitenFccs - ShockyuiflashNoch keine Bewertungen
- Drugs Acting On Cardiovascular SystemDokument81 SeitenDrugs Acting On Cardiovascular SystemevaNoch keine Bewertungen
- SupervisorsDokument1 SeiteSupervisorsBOOKREADER_NOW100% (2)
- Diagnosis & Management of Shock: SuriyadiDokument17 SeitenDiagnosis & Management of Shock: SuriyadiDeady NurdiantoNoch keine Bewertungen
- CARESCAPE Monitor B650: Clinical Reference ManualDokument210 SeitenCARESCAPE Monitor B650: Clinical Reference ManualJonathan ScottNoch keine Bewertungen
- Hypovolemic ShockDokument21 SeitenHypovolemic ShockOlga GoryachevaNoch keine Bewertungen
- Shock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentDokument64 SeitenShock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentHarika BandaruNoch keine Bewertungen
- Diagnosis and Management of ShockDokument31 SeitenDiagnosis and Management of ShockAmeliaNoch keine Bewertungen
- Diagnosis and Management of Shock: SHK 1 SHK 1Dokument27 SeitenDiagnosis and Management of Shock: SHK 1 SHK 1Agung NugrohoNoch keine Bewertungen
- Diagnosis Dan Manajemen SyokDokument22 SeitenDiagnosis Dan Manajemen SyokRatika Ayu PiliangNoch keine Bewertungen
- Kuliah Syok 2020 (DR Ahmad Yafiz Hasby SpAn)Dokument48 SeitenKuliah Syok 2020 (DR Ahmad Yafiz Hasby SpAn)RezaNoch keine Bewertungen
- Pemicu 1 KGD: Muhammad Fahmi Rosyadi 405140220Dokument137 SeitenPemicu 1 KGD: Muhammad Fahmi Rosyadi 405140220fahmi rosyadiNoch keine Bewertungen
- 1aAQ9K9el0XG34EBO27zATWpBZ9igCdV6 1Dokument23 Seiten1aAQ9K9el0XG34EBO27zATWpBZ9igCdV6 1Sonia khanNoch keine Bewertungen
- HypertensionDokument43 SeitenHypertensionAbin PNoch keine Bewertungen
- Haemorrhagic Shock, Resuscitation and HaemodynamicsDokument31 SeitenHaemorrhagic Shock, Resuscitation and HaemodynamicsNinaNoch keine Bewertungen
- Cardio Genic and Obstructive ShockDokument66 SeitenCardio Genic and Obstructive ShockdrkurniatiNoch keine Bewertungen
- Session 24 Heart FailureDokument15 SeitenSession 24 Heart Failuredreampurpose97Noch keine Bewertungen
- Approach To ShockDokument30 SeitenApproach To ShocktigistNoch keine Bewertungen
- Cardio Genic ShockDokument6 SeitenCardio Genic ShockDedy HartantoNoch keine Bewertungen
- Approach To Patient With HypertensionDokument64 SeitenApproach To Patient With HypertensionAndrassy Twinkle AlineaNoch keine Bewertungen
- Management of ShockDokument18 SeitenManagement of ShockObongsamuel IdiongNoch keine Bewertungen
- Penatalaksanaan SyokDokument59 SeitenPenatalaksanaan SyokArif NurfadhilahNoch keine Bewertungen
- Shock: Disampaikan Oleh: Dr. I G A G Utara Hartawan, Span MarsDokument88 SeitenShock: Disampaikan Oleh: Dr. I G A G Utara Hartawan, Span MarsNym Angga SantosaNoch keine Bewertungen
- Shock in Children Lecture NewDokument41 SeitenShock in Children Lecture NewDky HartonoNoch keine Bewertungen
- L15-Shock & Resuscitation LectureDokument49 SeitenL15-Shock & Resuscitation LectureYosra —Noch keine Bewertungen
- PBL 1Dokument111 SeitenPBL 1fahmi rosyadiNoch keine Bewertungen
- Shock: William Lawson, MD Division of Allergy, Pulmonary, and Critical Care MedicineDokument41 SeitenShock: William Lawson, MD Division of Allergy, Pulmonary, and Critical Care MedicinerohitNoch keine Bewertungen
- Shock Syndrome: DR Melkamu BDokument62 SeitenShock Syndrome: DR Melkamu BAsteway MesfinNoch keine Bewertungen
- NullDokument58 SeitenNullElteyb Nor eldaimNoch keine Bewertungen
- Terapi Cairan PediatriDokument74 SeitenTerapi Cairan PediatriAnonymous 0SYzMqje2100% (1)
- Arterial Blood Pressure RegulationDokument21 SeitenArterial Blood Pressure Regulationnaresh sharmaNoch keine Bewertungen
- Hypertension and Angina DrugsDokument158 SeitenHypertension and Angina DrugsMelissa SalayogNoch keine Bewertungen
- Vasoactive Drugs (PICUCOURSE)Dokument52 SeitenVasoactive Drugs (PICUCOURSE)surasuarezlopezNoch keine Bewertungen
- Shock in The Pediatric Patient: or Oxygen Don't Go Where The Blood Won't Flow!Dokument63 SeitenShock in The Pediatric Patient: or Oxygen Don't Go Where The Blood Won't Flow!Nishanth BabuNoch keine Bewertungen
- Manajemen ShockDokument47 SeitenManajemen ShockPutry RizqiaNoch keine Bewertungen
- Pharm CH 11 AntihypertensivesDokument42 SeitenPharm CH 11 AntihypertensivesDaniel AdamsNoch keine Bewertungen
- Cardiovascular Drugs 4Dokument31 SeitenCardiovascular Drugs 4ismailaiaibrahimNoch keine Bewertungen
- СердечнаяDokument70 SeitenСердечнаяDaniel FunkNoch keine Bewertungen
- Shock: in Multiple InjuryDokument32 SeitenShock: in Multiple InjuryNazirul HanifNoch keine Bewertungen
- Hypovolemic Shock Cardiogenic Shock Obstructive Shock: Prepared By: HO Tiviyah Mentor: DR Tiong Supervisor: DR Tham MinDokument29 SeitenHypovolemic Shock Cardiogenic Shock Obstructive Shock: Prepared By: HO Tiviyah Mentor: DR Tiong Supervisor: DR Tham MinTeik Wei TanNoch keine Bewertungen
- Lecture 6 Anti HypertensionDokument40 SeitenLecture 6 Anti HypertensionMNGS StudioNoch keine Bewertungen
- Vasoactive TherapyDokument26 SeitenVasoactive Therapylidya agustinNoch keine Bewertungen
- Pharmacology Semi FinalsDokument269 SeitenPharmacology Semi FinalsTrishaNoch keine Bewertungen
- Fluids and Electrolytes and Acid Base PhysiologyDokument64 SeitenFluids and Electrolytes and Acid Base PhysiologyJesserene Mangulad SorianoNoch keine Bewertungen
- Hypovolemic ShockDokument36 SeitenHypovolemic ShockRia CintyaNoch keine Bewertungen
- Pad HPNDokument137 SeitenPad HPNpmm21d229Noch keine Bewertungen
- Cardivascular DrugsDokument27 SeitenCardivascular DrugsYounas BhattiNoch keine Bewertungen
- Emergency Drugs: A Review: Jeselo O. Gorme, RNDokument71 SeitenEmergency Drugs: A Review: Jeselo O. Gorme, RNdodong skyroseNoch keine Bewertungen
- 10.15 Edrian Zulkarnain - ShockDokument42 Seiten10.15 Edrian Zulkarnain - ShockBintang UbamnataNoch keine Bewertungen
- Pulmonary Edema by DR Gireesh Kumar K PDokument16 SeitenPulmonary Edema by DR Gireesh Kumar K PAETCM Emergency medicineNoch keine Bewertungen
- Perspective Plan 2022-27Dokument57 SeitenPerspective Plan 2022-27So kharap kuchNoch keine Bewertungen
- ESTAVILLO, Karen G. (FEVER UTI, CONSTI)Dokument4 SeitenESTAVILLO, Karen G. (FEVER UTI, CONSTI)Karen EstavilloNoch keine Bewertungen
- Project CharterDokument9 SeitenProject CharterTatianaObregon100% (1)
- Telehealth Research and Evaluation Implications For Decision MakersDokument9 SeitenTelehealth Research and Evaluation Implications For Decision Makerscharlsandroid01Noch keine Bewertungen
- Rad 3 PDFDokument5 SeitenRad 3 PDFjovanaNoch keine Bewertungen
- Contraceptive Options For Women and Couples With HIV: Intrauterine Device (Iud or Iucd)Dokument23 SeitenContraceptive Options For Women and Couples With HIV: Intrauterine Device (Iud or Iucd)Sitha MahendrataNoch keine Bewertungen
- Damage Control Orthopaedics DR Bambang SpOT (Salinan Berkonflik Enggar Yusrina 2015-10-14)Dokument37 SeitenDamage Control Orthopaedics DR Bambang SpOT (Salinan Berkonflik Enggar Yusrina 2015-10-14)SemestaNoch keine Bewertungen
- Patient Safety and Quality Improvement 101Dokument81 SeitenPatient Safety and Quality Improvement 101Manasi PandaNoch keine Bewertungen
- 3 Speech and Language Therapy DDokument2 Seiten3 Speech and Language Therapy DBárbara FerreiraNoch keine Bewertungen
- Drug Study - AlleyahDokument10 SeitenDrug Study - AlleyahLorenzo, Alleyah Jaira D.Noch keine Bewertungen
- ENDOCRINE 1.3 Incidentallomas, Conn's SyndromeDokument5 SeitenENDOCRINE 1.3 Incidentallomas, Conn's SyndromeJem QuintoNoch keine Bewertungen
- Block 4 Lung PathDokument31 SeitenBlock 4 Lung PathShalini ShanmugalingamNoch keine Bewertungen
- CsaDokument10 SeitenCsaBEATRIZ CUBILLONoch keine Bewertungen
- Cefotaxime and Ceftriaxone PDFDokument7 SeitenCefotaxime and Ceftriaxone PDFDwi FitriyaniNoch keine Bewertungen
- A 25-Year-Old Man With New-Onset Seizures PDFDokument8 SeitenA 25-Year-Old Man With New-Onset Seizures PDFMr. LNoch keine Bewertungen
- KyphosisDokument3 SeitenKyphosismnatuelNoch keine Bewertungen
- Drug Regulations in India DR Surinder SinghDokument29 SeitenDrug Regulations in India DR Surinder SinghnutelladdictNoch keine Bewertungen
- Varicose Veins Diagnosis and TreatmentDokument7 SeitenVaricose Veins Diagnosis and Treatmenthossein kasiriNoch keine Bewertungen
- EU Digital COVID Certificate Certificat Digital European COVIDDokument2 SeitenEU Digital COVID Certificate Certificat Digital European COVIDDespre FotografieNoch keine Bewertungen
- Advancement in The Recently Development of Sublingual Tablet For Various Diseases A ReviewDokument7 SeitenAdvancement in The Recently Development of Sublingual Tablet For Various Diseases A ReviewEditor IJTSRDNoch keine Bewertungen
- Primary HyperparathyroidismDokument9 SeitenPrimary HyperparathyroidismJamesNoch keine Bewertungen
- Drug Regulatory Agency of Pakistan (DRAP)Dokument12 SeitenDrug Regulatory Agency of Pakistan (DRAP)Mrs YezdaniNoch keine Bewertungen
- Medicinecomplete Clark Drug and PoisonDokument25 SeitenMedicinecomplete Clark Drug and PoisonArménio SantosNoch keine Bewertungen