Das könnte Ihnen auch gefallen
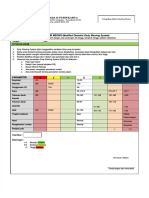
- Formulir Meows (FORMULIR MEOWS (Modified Obstetric Early Warning System Modified Obstetric Early Warning System) )Dokument2 SeitenFormulir Meows (FORMULIR MEOWS (Modified Obstetric Early Warning System Modified Obstetric Early Warning System) )miraNoch keine Bewertungen
- Manajemen HipertensiDokument46 SeitenManajemen HipertensiYeni BelawatiNoch keine Bewertungen
- Perlindungan Hukum Terhadap Peserta BpjsDokument22 SeitenPerlindungan Hukum Terhadap Peserta BpjsRizal Saputra100% (1)
- Mengapa Kesehatan Reproduksi Itu Penting - Paparan Deputi KBKRDokument14 SeitenMengapa Kesehatan Reproduksi Itu Penting - Paparan Deputi KBKRMoch Yuzjiandi AL-Ghifari100% (1)
- Tabel Referensi Diagnosa Non SpesialistikDokument12 SeitenTabel Referensi Diagnosa Non SpesialistikDian SunartiNoch keine Bewertungen
- Form Ringkasan Perawatan Pasien Pulang (Resume Medis)Dokument1 SeiteForm Ringkasan Perawatan Pasien Pulang (Resume Medis)gandi mahardika muktiNoch keine Bewertungen
- Terapi Hipertensi (Hipertensi Ve Disease) : Dr. Fitri SeptianingsihDokument23 SeitenTerapi Hipertensi (Hipertensi Ve Disease) : Dr. Fitri SeptianingsihMaulana HasanNoch keine Bewertungen
- Left Ventricular Hyperthrophy CriteriaDokument2 SeitenLeft Ventricular Hyperthrophy CriteriaDya AndryanNoch keine Bewertungen
- Daftar Pustaka Hipertensi Pada Usia MudaDokument10 SeitenDaftar Pustaka Hipertensi Pada Usia MudaToby Hadinata WiranegaraNoch keine Bewertungen
- SOP Cutaneus Larva Migran 1Dokument2 SeitenSOP Cutaneus Larva Migran 1Muhammad IqbalNoch keine Bewertungen
- Kliping Kasus Pelanggaran Ham Di IndonesiaDokument7 SeitenKliping Kasus Pelanggaran Ham Di IndonesiaKhaerudinClasMildNoch keine Bewertungen
- Blanko Permintaan Pemeriksaan RadiologiDokument4 SeitenBlanko Permintaan Pemeriksaan Radiologijoko suhartonoNoch keine Bewertungen
- Jurnal Pisang Ambon Pada Hipertensi PDFDokument6 SeitenJurnal Pisang Ambon Pada Hipertensi PDFVivoraroNoch keine Bewertungen
- National Cholesterol Education Program: Adult Treatment Panel III (ATP III) GuidelinesDokument103 SeitenNational Cholesterol Education Program: Adult Treatment Panel III (ATP III) GuidelinesAdil AhmedNoch keine Bewertungen
- FL Leaflet Napza FixDokument2 SeitenFL Leaflet Napza FixDesii NainggolanNoch keine Bewertungen
- 7.2.3.a Sop TriageDokument2 Seiten7.2.3.a Sop TriageBuce SabilNoch keine Bewertungen
- File 1593308213Dokument92 SeitenFile 1593308213NURSIAH ALMAULIDANoch keine Bewertungen
- HERBALIFEDokument1 SeiteHERBALIFEAbdulHakimSallehNoch keine Bewertungen
- Tabel ICD 10 English Indonesia LengkapDokument432 SeitenTabel ICD 10 English Indonesia LengkaptwindaNoch keine Bewertungen
- Leaflet Diare - VincentDokument2 SeitenLeaflet Diare - VincenternaNoch keine Bewertungen
- Advance Care Planning English VersionDokument9 SeitenAdvance Care Planning English VersionAlma NurfitriaNoch keine Bewertungen
- COPD - Update Diagnosis and Management of Stable COPDDokument29 SeitenCOPD - Update Diagnosis and Management of Stable COPDIwanNoch keine Bewertungen
- Ambiguous GenitaliaDokument47 SeitenAmbiguous GenitaliaDrvsowmya Lakshmi100% (1)
- Formulir Laporan Insiden Internal Di PuskesmasDokument3 SeitenFormulir Laporan Insiden Internal Di Puskesmassandal sanglirNoch keine Bewertungen
- Resusitasi Jantung Paru Berkualitas: Dr. Ichwan Zuanto 3 FEBRUARI 2018 Rsia Setya BhaktiDokument12 SeitenResusitasi Jantung Paru Berkualitas: Dr. Ichwan Zuanto 3 FEBRUARI 2018 Rsia Setya BhaktiIchwan Zuanto SjamanNoch keine Bewertungen
- Kel 3 TPNDokument32 SeitenKel 3 TPNTriliantari Siregar0% (1)
- Sungai BaungDokument390 SeitenSungai BaungHeri JumardiNoch keine Bewertungen
- Algoritma DkaDokument1 SeiteAlgoritma DkaKang KangNoch keine Bewertungen
- Demam Berdarah Dengue Pada Anak: MustaringDokument70 SeitenDemam Berdarah Dengue Pada Anak: MustaringHabi Septiati MusinNoch keine Bewertungen
- Sop Common ColdDokument1 SeiteSop Common ColdEma Maudina LestariNoch keine Bewertungen
- Jurnal ProlanisDokument10 SeitenJurnal ProlanisSuci MayveraNoch keine Bewertungen
- LBP Form No. 2 RevisedDokument80 SeitenLBP Form No. 2 RevisedJhumar YuNoch keine Bewertungen
- Jadwal Posyandu Lansia SeptemberDokument3 SeitenJadwal Posyandu Lansia SeptemberNurmilaNoch keine Bewertungen
- Kode Icd XDokument9 SeitenKode Icd XRini YuniartiNoch keine Bewertungen
- COREQ Untuk KualitatifDokument9 SeitenCOREQ Untuk KualitatifNurul QalbyNoch keine Bewertungen
- Bango MaretDokument280 SeitenBango MaretTisa KimNoch keine Bewertungen
- Leaflet Jiwa 2Dokument2 SeitenLeaflet Jiwa 2Lela Nazila ItuSayaNoch keine Bewertungen
- Diare Akut: Adhesi Invasi Sitotoksin EnterotoksinDokument4 SeitenDiare Akut: Adhesi Invasi Sitotoksin EnterotoksinVeronica Yosita AnandaNoch keine Bewertungen
- RJP Aha 2020Dokument29 SeitenRJP Aha 2020byeukid_224862614Noch keine Bewertungen
- ESC Arterial Hypertension 2018Dokument98 SeitenESC Arterial Hypertension 2018ddantoniusgmailNoch keine Bewertungen
- Resume Pre HemodialisaDokument4 SeitenResume Pre HemodialisaPutra RahmatNoch keine Bewertungen
- Bench Top Centrifuge User'S ManualDokument18 SeitenBench Top Centrifuge User'S ManualAleksey AleksNoch keine Bewertungen
- Lampiran Kode DiagnosaDokument7 SeitenLampiran Kode DiagnosamulyaniNoch keine Bewertungen
- 4869 2 7 Tabel Angka Main Syd SGP HKG: InputDokument63 Seiten4869 2 7 Tabel Angka Main Syd SGP HKG: InputHeri Pam-pam PriyadiNoch keine Bewertungen
- Medical Check Up: Cek KesehatanDokument20 SeitenMedical Check Up: Cek KesehatanEmi PephiNoch keine Bewertungen
- Upt Puskesmas Batang Kuis: Bells' PalsyDokument5 SeitenUpt Puskesmas Batang Kuis: Bells' PalsyMuhammad IqbalNoch keine Bewertungen
- Jurnal SIK Pengembangan SIKNAS Di Lampung 2018Dokument16 SeitenJurnal SIK Pengembangan SIKNAS Di Lampung 2018ELLIYAWATINoch keine Bewertungen
- HIPERTENSI LANSIAaDokument88 SeitenHIPERTENSI LANSIAaMuzayyanatulhayat ARNoch keine Bewertungen
- Glomerulonephritis-1 (Dr. Soffa)Dokument58 SeitenGlomerulonephritis-1 (Dr. Soffa)Rahmailla Khanza Diana FebriliantriNoch keine Bewertungen
- GLOMERULONEPHRITIS (Bright's Disease)Dokument8 SeitenGLOMERULONEPHRITIS (Bright's Disease)Anjitha K. JNoch keine Bewertungen
- GlomerulonephritisDokument59 SeitenGlomerulonephritistressNoch keine Bewertungen
- Nephrotic Syndrome-1Dokument21 SeitenNephrotic Syndrome-1Wondimu EliasNoch keine Bewertungen
- Nephritic Syndrome - Armando HasudunganDokument14 SeitenNephritic Syndrome - Armando HasudunganzahraaNoch keine Bewertungen
- Glomerulonefritis Akut Dan Kronis: DR - Hasan Basri, Sppd-Kgh-FinasimDokument53 SeitenGlomerulonefritis Akut Dan Kronis: DR - Hasan Basri, Sppd-Kgh-FinasimnadddNoch keine Bewertungen
- GLOMERULOPATHYDokument51 SeitenGLOMERULOPATHYAumnissa SamsiNoch keine Bewertungen
- Nephrotic SyndromeDokument5 SeitenNephrotic SyndromeAnjhiene CambaNoch keine Bewertungen
- Glomerulonephritis 2Dokument56 SeitenGlomerulonephritis 2Mans FansNoch keine Bewertungen
- Glomerulopathies: Hasyim Kasim Divisi Nephrology and Hypertensi FKUH 2016Dokument39 SeitenGlomerulopathies: Hasyim Kasim Divisi Nephrology and Hypertensi FKUH 2016andiNoch keine Bewertungen
- Nephrotic Vs Nephritic SyndromeDokument80 SeitenNephrotic Vs Nephritic Syndromevan016_bunnyNoch keine Bewertungen
- Glomerulonephritis: Nameesha Natasha Naidu 20130105Dokument26 SeitenGlomerulonephritis: Nameesha Natasha Naidu 20130105AliMalikNoch keine Bewertungen
- Respiration 3Dokument23 SeitenRespiration 3api-19916399100% (1)
- Physiology - Retired QuestionsDokument12 SeitenPhysiology - Retired Questionsapi-19916399Noch keine Bewertungen
- Respiration TwoDokument58 SeitenRespiration Twoapi-19916399Noch keine Bewertungen
- Blood CoagulationDokument70 SeitenBlood Coagulationapi-19916399Noch keine Bewertungen
- Preload and AfterloadDokument28 SeitenPreload and Afterloadapi-19916399100% (1)
- Nervous System 7Dokument20 SeitenNervous System 7api-19916399Noch keine Bewertungen
- Physiology of Blood VesselDokument65 SeitenPhysiology of Blood Vesselapi-19916399Noch keine Bewertungen
- Gastrointestinal PhysiologyDokument134 SeitenGastrointestinal Physiologyapi-19916399100% (1)
- Physiology Answers and ExDokument19 SeitenPhysiology Answers and Exapi-19916399Noch keine Bewertungen
- Nervous System 6Dokument27 SeitenNervous System 6api-19916399Noch keine Bewertungen
- Jingying T.A. Department of PhysiologyDokument19 SeitenJingying T.A. Department of Physiologyapi-19916399Noch keine Bewertungen
- Jingying T.A. Department of PhysiologyDokument26 SeitenJingying T.A. Department of Physiologyapi-19916399Noch keine Bewertungen
- Jingying T.A. Department of PhysiologyDokument22 SeitenJingying T.A. Department of Physiologyapi-19916399Noch keine Bewertungen
- Neurophysiology: Run Fight Speak Think Watch Listen Taste SmellDokument22 SeitenNeurophysiology: Run Fight Speak Think Watch Listen Taste Smellapi-19916399Noch keine Bewertungen
- 01.introduction To PhysiologyDokument44 Seiten01.introduction To Physiologyapi-19916399Noch keine Bewertungen
- Evaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac IndexDokument53 SeitenEvaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac Indexapi-19916399Noch keine Bewertungen
- Gastrointestinal PhysiologDokument133 SeitenGastrointestinal Physiologapi-19916399100% (1)
- Electrophysiological Properties of Cardiac MyocytesDokument39 SeitenElectrophysiological Properties of Cardiac Myocytesapi-19916399Noch keine Bewertungen
- Physiology of Blood VesselDokument65 SeitenPhysiology of Blood Vesselapi-19916399Noch keine Bewertungen
- Electrical Activity of The HeartDokument29 SeitenElectrical Activity of The Heartapi-19916399Noch keine Bewertungen
- Evaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac IndexDokument53 SeitenEvaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac Indexapi-19916399Noch keine Bewertungen
- Chapter 2 - 1 - ForeignerDokument35 SeitenChapter 2 - 1 - Foreignerapi-19916399Noch keine Bewertungen
- Circulation4 5Dokument1 SeiteCirculation4 5api-19916399Noch keine Bewertungen
- Kyuhyun Wang, MD: What Is The Rhythm?Dokument43 SeitenKyuhyun Wang, MD: What Is The Rhythm?api-19916399Noch keine Bewertungen
- Rhythmical Excitation of The HeartDokument29 SeitenRhythmical Excitation of The Heartapi-19916399Noch keine Bewertungen
- Use of Autism Diagnostic Interview1 Adi R in Clinical PracticeDokument1 SeiteUse of Autism Diagnostic Interview1 Adi R in Clinical Practiceaspire centerNoch keine Bewertungen
- Volunteer Report FinalDokument11 SeitenVolunteer Report FinalBeenish JehangirNoch keine Bewertungen
- Primary Health CentreDokument22 SeitenPrimary Health CentreRakersh Patidar100% (1)
- My Hands The Body Is Painful / Do ROM Actions Done With MyDokument3 SeitenMy Hands The Body Is Painful / Do ROM Actions Done With MyHanip Little-FaqotNoch keine Bewertungen
- Antihypnotics and AnxiolyticsDokument12 SeitenAntihypnotics and AnxiolyticsSabreena NordinNoch keine Bewertungen
- Bacteria Vs Viruses and DiseasesDokument38 SeitenBacteria Vs Viruses and DiseasesNha HoangNoch keine Bewertungen
- Types, Characteristics, and Identification of Learners With Difficulty Seeing - 0Dokument13 SeitenTypes, Characteristics, and Identification of Learners With Difficulty Seeing - 0Laleth Mendoza OjalesNoch keine Bewertungen
- The Human Heart: © 2014 Pearson Education, IncDokument45 SeitenThe Human Heart: © 2014 Pearson Education, IncSafee HaiderNoch keine Bewertungen
- 09 Marijuana Facts For TeensDokument24 Seiten09 Marijuana Facts For Teensapi-309082881Noch keine Bewertungen
- Radiance TechniqueDokument37 SeitenRadiance TechniqueMokhtar Mohd100% (1)
- Cardiology: Nature ReviewsDokument15 SeitenCardiology: Nature ReviewsluonganhsiNoch keine Bewertungen
- Logbookgazett MOHDokument56 SeitenLogbookgazett MOHShima OnnNoch keine Bewertungen
- Anesthesia For in Vitro Fertilization: Review ArticleDokument11 SeitenAnesthesia For in Vitro Fertilization: Review ArticleSumangala MagiNoch keine Bewertungen
- The Digestive System: Maria Victoria M. Villarica MD OLFU College of Medicine Department of PediatricsDokument81 SeitenThe Digestive System: Maria Victoria M. Villarica MD OLFU College of Medicine Department of PediatricsSven OrdanzaNoch keine Bewertungen
- AARC Clinical Practice GuidelineDokument7 SeitenAARC Clinical Practice GuidelineXime GonzálezNoch keine Bewertungen
- 017 Pathology MCQ ACEM Primary GITDokument3 Seiten017 Pathology MCQ ACEM Primary GITRebeenMustafaNoch keine Bewertungen
- 5 Day Fast by Bo Sanchez PDFDokument14 Seiten5 Day Fast by Bo Sanchez PDFBelle100% (1)
- Chapter 4 Factors Affecting Performance: Training Purpose OnlyDokument19 SeitenChapter 4 Factors Affecting Performance: Training Purpose OnlySajjad ShamimNoch keine Bewertungen
- Bio Printing Biology Oral PresentationDokument15 SeitenBio Printing Biology Oral PresentationVanessa Carmody100% (1)
- IvpbhandoutDokument2 SeitenIvpbhandoutapi-283303129Noch keine Bewertungen
- FRE - L3 Core Terminology - 2018Dokument28 SeitenFRE - L3 Core Terminology - 2018RahulNoch keine Bewertungen
- Summer 2122 Aubf Lab Periodical Test 2Dokument38 SeitenSummer 2122 Aubf Lab Periodical Test 2RuchieNoch keine Bewertungen
- Artificial IntelligenceDokument27 SeitenArtificial IntelligenceMd HassanNoch keine Bewertungen
- Importance of Espresso Coffee Machine ParametersDokument10 SeitenImportance of Espresso Coffee Machine ParametersOssian89Noch keine Bewertungen
- Top 10 Differential Diagnoses in Family Medicine - CoughDokument2 SeitenTop 10 Differential Diagnoses in Family Medicine - CoughTiza OyonNoch keine Bewertungen
- Cysteamine - Full Profile - 170917Dokument11 SeitenCysteamine - Full Profile - 170917Walter MendozaNoch keine Bewertungen
- Dental ImplantsDokument1 SeiteDental ImplantsPaWan VelagaNoch keine Bewertungen
- Genetic Analysis of Rare Disease: A Bioinformatic ApproachDokument55 SeitenGenetic Analysis of Rare Disease: A Bioinformatic Approachparetini01Noch keine Bewertungen
- Nur 102Dokument3 SeitenNur 102Fretchel Grace Silverado MesaNoch keine Bewertungen
- Clinical Teaching 4PEUPERAL SEPSISDokument5 SeitenClinical Teaching 4PEUPERAL SEPSISAjit M Prasad Prasad100% (1)