Das könnte Ihnen auch gefallen
- Multiple Myeloma: LT Col Vivek AggarwalDokument42 SeitenMultiple Myeloma: LT Col Vivek AggarwalShravan Rakaraddi100% (2)
- Multiple Myeloma PreparedDokument54 SeitenMultiple Myeloma PreparedSathyadharan PaneerNoch keine Bewertungen
- Cases Study in Plasma Cell DyscrasiaDokument87 SeitenCases Study in Plasma Cell Dyscrasiadrafq2000Noch keine Bewertungen
- Multiple Myeloma and Related Disorders: Kumar RajagopalanDokument71 SeitenMultiple Myeloma and Related Disorders: Kumar RajagopalananaskabahaNoch keine Bewertungen
- AL Amyloidosis Presenting As Inflammatory PolyarthritisDokument33 SeitenAL Amyloidosis Presenting As Inflammatory PolyarthritisShoaib MomenNoch keine Bewertungen
- Plasma Cell DyscrasiasDokument68 SeitenPlasma Cell Dyscrasiassarath chandranNoch keine Bewertungen
- Multiple Myeloma: Dr. Utsav AgrawalDokument23 SeitenMultiple Myeloma: Dr. Utsav AgrawalWaris ZegaNoch keine Bewertungen
- Plasma Cell Dyscrasia: Sri Kartika SariDokument35 SeitenPlasma Cell Dyscrasia: Sri Kartika SariSelimatul AlpaeniNoch keine Bewertungen
- Dr. Tika - PLASMA CELL DYSCRASIADokument36 SeitenDr. Tika - PLASMA CELL DYSCRASIAKantorCamat TaliwangNoch keine Bewertungen
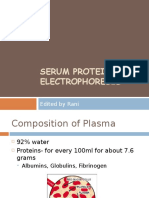
- Serum Protein Electrophoresis: Edited by RaniDokument66 SeitenSerum Protein Electrophoresis: Edited by RaniMustakim DuharingNoch keine Bewertungen
- Multiple Myeloma and Related Conditions: Conditions Associated With M Proteins Stable ProductionDokument28 SeitenMultiple Myeloma and Related Conditions: Conditions Associated With M Proteins Stable ProductionmedicinefaezNoch keine Bewertungen
- Multiple Myeloma and Understanding Your LabsDokument44 SeitenMultiple Myeloma and Understanding Your LabsAfaq AhmadNoch keine Bewertungen
- Netter's Internal Medicine 2nd Ed 14Dokument6 SeitenNetter's Internal Medicine 2nd Ed 14Panagiotis SouldatosNoch keine Bewertungen
- Multiple Myeloma A New Treatment ApproachDokument27 SeitenMultiple Myeloma A New Treatment ApproachIndonesian Journal of Cancer100% (1)
- Nephrotic SyndromeDokument24 SeitenNephrotic SyndromeSamah KhanNoch keine Bewertungen
- Plasma Cell DyscrasiasDokument10 SeitenPlasma Cell DyscrasiasRazib HasanNoch keine Bewertungen
- Plasma Cell DisordersDokument67 SeitenPlasma Cell DisordersAmbarsari Kusuma NingtyasNoch keine Bewertungen
- Laboratorial Diagnostics Keypoints RevisionDokument6 SeitenLaboratorial Diagnostics Keypoints RevisionFathimathNoch keine Bewertungen
- Myeloma StudyDokument3 SeitenMyeloma Study5dbcyqr4m4Noch keine Bewertungen
- Dickvet What Diagnosis April 2014Dokument6 SeitenDickvet What Diagnosis April 2014VioletNoch keine Bewertungen
- Immunoprolifearative and Immunodeficiency and Tumor ImmunologyDokument62 SeitenImmunoprolifearative and Immunodeficiency and Tumor ImmunologysssahilzNoch keine Bewertungen
- Lecture 10 - Plasma Proteins - 18 Sep 2006Dokument34 SeitenLecture 10 - Plasma Proteins - 18 Sep 2006api-3703352100% (3)
- Nephrotic Syndrome in Adult (Bahan Kuliah)Dokument49 SeitenNephrotic Syndrome in Adult (Bahan Kuliah)Jkp PhieNoch keine Bewertungen
- Nephrotic Syndrome: Jaiganesh.M, M.D (General Medicine) Asst. Professor, S.M.C.HDokument60 SeitenNephrotic Syndrome: Jaiganesh.M, M.D (General Medicine) Asst. Professor, S.M.C.HJaiganesh MuruganandamNoch keine Bewertungen
- 7.21.09 Kruska Multiple MyelomaDokument15 Seiten7.21.09 Kruska Multiple MyelomaAfaq AhmadNoch keine Bewertungen
- Plasma Proteins in Disease DiagnosisDokument81 SeitenPlasma Proteins in Disease DiagnosisSaaqo Qasim100% (1)
- Post PregnantDokument27 SeitenPost PregnantShreyas RavishankarNoch keine Bewertungen
- Aplastic AnemiaDokument6 SeitenAplastic AnemiaLargactil CpzNoch keine Bewertungen
- Plasma ProteinsDokument23 SeitenPlasma ProteinsNgonie Dube100% (1)
- Multiple MyelomaDokument15 SeitenMultiple MyelomaDinda YusditiraNoch keine Bewertungen
- Anemia-2: Overview and Select Cases: Marc Zumberg Associate Professor Division of Hematology/OncologyDokument95 SeitenAnemia-2: Overview and Select Cases: Marc Zumberg Associate Professor Division of Hematology/OncologyDenise CssNoch keine Bewertungen
- Multiple Mieloma Dan PVDokument20 SeitenMultiple Mieloma Dan PVariienndrrahanniieNoch keine Bewertungen
- Membranous Nephropathy - Case ReportDokument8 SeitenMembranous Nephropathy - Case ReportArundhatiNoch keine Bewertungen
- Aplastic Anemia: Edited: Dr. Dairion Gatot SP - PD-KHOMDokument11 SeitenAplastic Anemia: Edited: Dr. Dairion Gatot SP - PD-KHOMrubyniNoch keine Bewertungen
- Slide Microteaching MM Iqbal 2Dokument40 SeitenSlide Microteaching MM Iqbal 2RAJA HARAHAPNoch keine Bewertungen
- Anemia Workshop1Dokument80 SeitenAnemia Workshop1api-3762917Noch keine Bewertungen
- Serum Protein ElectrophoresisDokument7 SeitenSerum Protein ElectrophoresisShahrulnizam SaudiNoch keine Bewertungen
- Serum Protein Electrophoresis & Their Clinical ImportanceDokument44 SeitenSerum Protein Electrophoresis & Their Clinical ImportanceDr. M. Prasad NaiduNoch keine Bewertungen
- A Review of GAUCHER DiseaseDokument47 SeitenA Review of GAUCHER DiseasemaleehaNoch keine Bewertungen
- Lymphocytic Leukemia in A Golden Retriever Dog - A Case ReportDokument14 SeitenLymphocytic Leukemia in A Golden Retriever Dog - A Case ReportGanesh DasaraNoch keine Bewertungen
- Monoclonal GammopathiesDokument70 SeitenMonoclonal GammopathiesElisa Lincă100% (1)
- Lymphocytic Leukemia in A Golden Retriever Dog - A CaseDokument14 SeitenLymphocytic Leukemia in A Golden Retriever Dog - A CaseGanesh DasaraNoch keine Bewertungen
- Multiple MyelomaDokument34 SeitenMultiple Myelomad clarkeNoch keine Bewertungen
- Ditorials Erspectives: David C. Seldin, Vaishali SanchorawalaDokument5 SeitenDitorials Erspectives: David C. Seldin, Vaishali Sanchorawalasalmamaged7619Noch keine Bewertungen
- Final Hem and Onc Slides39 EndDokument50 SeitenFinal Hem and Onc Slides39 EndiniidzniNoch keine Bewertungen
- Multiple MyelomaDokument23 SeitenMultiple Myelomabubbu92Noch keine Bewertungen
- The Many Faces of Monoclonal GammopathiesDokument44 SeitenThe Many Faces of Monoclonal GammopathiesimagigatoNoch keine Bewertungen
- LO TambahanDokument5 SeitenLO TambahanDapot SianiparNoch keine Bewertungen
- A Curious Case of QuadriplegiaDokument4 SeitenA Curious Case of QuadriplegiaInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Abetalipoproteinemia The Egyptian Journal of Medical Human GeneticsDokument4 SeitenAbetalipoproteinemia The Egyptian Journal of Medical Human Geneticsanisa auliaNoch keine Bewertungen
- Plasma Cell Dyscrasias: Miten R. Patel, MD Cancer Specialists of North FloridaDokument41 SeitenPlasma Cell Dyscrasias: Miten R. Patel, MD Cancer Specialists of North FloridaDr MonikaNoch keine Bewertungen
- Haematology 2020 PDFDokument131 SeitenHaematology 2020 PDFNaman GuptaNoch keine Bewertungen
- Plasma Cell NeoplasmsDokument36 SeitenPlasma Cell Neoplasmsdrafq2000Noch keine Bewertungen
- DK Gastro KonsulDokument48 SeitenDK Gastro Konsuldenina setyaNoch keine Bewertungen
- Chapter 6 Diagnostic EnzymologyDokument81 SeitenChapter 6 Diagnostic EnzymologyFathimathNoch keine Bewertungen
- Arciaga, FG - SGDPara 051221Dokument4 SeitenArciaga, FG - SGDPara 051221FG ArciagaNoch keine Bewertungen
- A Rare Case of Acute Pancreatitis Following Neurotoxic Snake EnvenomationDokument4 SeitenA Rare Case of Acute Pancreatitis Following Neurotoxic Snake EnvenomationSanjeevNoch keine Bewertungen
- Clinical ChemistryDokument12 SeitenClinical ChemistryClark Lopez100% (1)
- Monoclonal Gammopathies of Clinical SignificanceDokument9 SeitenMonoclonal Gammopathies of Clinical SignificanceSabrina DaidNoch keine Bewertungen
- 68th AACC Annual Scientific Meeting Abstract eBookVon Everand68th AACC Annual Scientific Meeting Abstract eBookNoch keine Bewertungen
- ADMA 2010 BlackboardDokument41 SeitenADMA 2010 Blackboardmonday125Noch keine Bewertungen
- Uric AcidDokument6 SeitenUric Acidmonday125100% (1)
- Caffeine BronchodilatorDokument30 SeitenCaffeine Bronchodilatormonday125Noch keine Bewertungen
- Pleasing Her Husband's Boss (Hot Wife and Her Cuckold 2) by Michaels DeanaDokument29 SeitenPleasing Her Husband's Boss (Hot Wife and Her Cuckold 2) by Michaels Deanamonday12560% (10)
- Clinical Guideline For Anticoagulant Use in AdultsDokument108 SeitenClinical Guideline For Anticoagulant Use in Adultsmonday125Noch keine Bewertungen
- ICP-MS Talk ACBDokument31 SeitenICP-MS Talk ACBmonday125Noch keine Bewertungen
- Bible 2018Dokument183 SeitenBible 2018monday125Noch keine Bewertungen
- 2010 - Zhang - EAP For AR Review PDFDokument8 Seiten2010 - Zhang - EAP For AR Review PDFmonday125Noch keine Bewertungen
- Karen Smith Duty Biochemist ScenariosDokument43 SeitenKaren Smith Duty Biochemist Scenariosmonday125100% (2)
- ST Agnes Catholic Primary SchoolDokument12 SeitenST Agnes Catholic Primary Schoolmonday125Noch keine Bewertungen
- FRCPath Cases 1Dokument36 SeitenFRCPath Cases 1monday125100% (1)
- Writing An Abstract: Sally - Benton@bartshealth - Nhs.ukDokument7 SeitenWriting An Abstract: Sally - Benton@bartshealth - Nhs.ukmonday125Noch keine Bewertungen
- FRCPath OSPE 25042014Dokument11 SeitenFRCPath OSPE 25042014monday125Noch keine Bewertungen
- OspeDokument29 SeitenOspemonday125Noch keine Bewertungen
- Critical Appraisal: DR A C J Hutchesson Chair of Examiners' Panel, Frcpath (Clinical Biochemistry)Dokument10 SeitenCritical Appraisal: DR A C J Hutchesson Chair of Examiners' Panel, Frcpath (Clinical Biochemistry)monday125Noch keine Bewertungen
- FOCUS SAS Training Day Leeds Dr. Joanna Sheldon Protein Reference Unit, St. George'sDokument19 SeitenFOCUS SAS Training Day Leeds Dr. Joanna Sheldon Protein Reference Unit, St. George'smonday125Noch keine Bewertungen
- Model Albumin AnswerDokument13 SeitenModel Albumin Answermonday125Noch keine Bewertungen
- FRCPath Chemical Pathology CurriculumDokument109 SeitenFRCPath Chemical Pathology Curriculummonday125Noch keine Bewertungen
- Frances Boa Methodology QuestionDokument39 SeitenFrances Boa Methodology Questionmonday125Noch keine Bewertungen
- Bill Bartlett - 1 1 1Dokument68 SeitenBill Bartlett - 1 1 1monday125Noch keine Bewertungen
- Master Sheet: 1. Irregular ClotDokument20 SeitenMaster Sheet: 1. Irregular Clotmonday125Noch keine Bewertungen
- Protein Electrophoresis, Immunofixation, and Immunodisplacement in Clinical Diagnosis. 2nd Edition, May 2011Dokument182 SeitenProtein Electrophoresis, Immunofixation, and Immunodisplacement in Clinical Diagnosis. 2nd Edition, May 2011Zia Uddin100% (3)
- Netter's Internal Medicine 2nd Ed 14Dokument6 SeitenNetter's Internal Medicine 2nd Ed 14Panagiotis SouldatosNoch keine Bewertungen
- Haematological Malignancies: Approach and Update.: Andrew Zolani Cakana. Professor of HaematologyDokument123 SeitenHaematological Malignancies: Approach and Update.: Andrew Zolani Cakana. Professor of HaematologyThomas MutanikwaNoch keine Bewertungen
- Katzmann - Leukaemia 2013Dokument5 SeitenKatzmann - Leukaemia 2013Carina MoitaNoch keine Bewertungen
- Diagnostic Approach To The Patient With Newly Identified Chronic Kidney DiseaseDokument1 SeiteDiagnostic Approach To The Patient With Newly Identified Chronic Kidney DiseaseLauraNoch keine Bewertungen
- Haematology 2020 PDFDokument131 SeitenHaematology 2020 PDFNaman GuptaNoch keine Bewertungen
- Multiple Myeloma Case StudyDokument42 SeitenMultiple Myeloma Case StudyHope Serquiña100% (2)
- Systemic Amyloidosis in Primary Hyperparathyroidism. Kam Newman, Mojtaba Akhtari, Salim Shackour, Ajit KesaniDokument1 SeiteSystemic Amyloidosis in Primary Hyperparathyroidism. Kam Newman, Mojtaba Akhtari, Salim Shackour, Ajit KesanijingerbrunoNoch keine Bewertungen
- Data Interpretation For Medical StudentDokument18 SeitenData Interpretation For Medical StudentWee K WeiNoch keine Bewertungen
- 600R003137 Cured WEB PDFDokument545 Seiten600R003137 Cured WEB PDFEdie M Murgia100% (9)
- Plasma Cell Dyscrasias: Miten R. Patel, MD Cancer Specialists of North FloridaDokument41 SeitenPlasma Cell Dyscrasias: Miten R. Patel, MD Cancer Specialists of North FloridaDr MonikaNoch keine Bewertungen
- Case Study MM-2Dokument40 SeitenCase Study MM-2Aya Sayed100% (1)
- Bahan Referat MMDokument29 SeitenBahan Referat MMTri Yudha NugrahaNoch keine Bewertungen
- Plasma Cell DyscrasiasDokument6 SeitenPlasma Cell DyscrasiasharideepNoch keine Bewertungen
- SMLEQBank 7th - 27-12-15 PDFDokument527 SeitenSMLEQBank 7th - 27-12-15 PDFIndrajit Barua100% (3)
- ImmunofixationDokument36 SeitenImmunofixationAstrianti Kusuma Wardani100% (1)
- SMLEQBank 15-12-15 PDFDokument294 SeitenSMLEQBank 15-12-15 PDFIndrajit Barua0% (2)
- Understanding and Interpreting The Serum Protein Electrophoresis - American Family Physician PDFDokument7 SeitenUnderstanding and Interpreting The Serum Protein Electrophoresis - American Family Physician PDFvmsNoch keine Bewertungen
- Monoclonal GammopathyDokument30 SeitenMonoclonal GammopathyGawri AbeyNoch keine Bewertungen
- Curcumin Role in ParaproteinemiaDokument18 SeitenCurcumin Role in ParaproteinemiaINDIRAKALYANINoch keine Bewertungen
- Haematology Handbook: Division of Specialty MedicineDokument30 SeitenHaematology Handbook: Division of Specialty MedicineAlina DumitracheNoch keine Bewertungen
- Case of Enlarged Hard TongueDokument13 SeitenCase of Enlarged Hard TongueKawther AbdallahNoch keine Bewertungen
- American Board of Family MedicineDokument66 SeitenAmerican Board of Family MedicineEhab Elkady100% (3)
- Plasma Cell DyscrasiasDokument21 SeitenPlasma Cell DyscrasiasJubril ZipamohNoch keine Bewertungen
- Multiple MyelomaDokument23 SeitenMultiple MyelomaRameshKrishnanNoch keine Bewertungen
- Data Interpretation For Medical Students PDFDokument905 SeitenData Interpretation For Medical Students PDFMarNoch keine Bewertungen
- POEMS SyndromeDokument13 SeitenPOEMS SyndromeFernando Suarez ChumaceroNoch keine Bewertungen
- Katzmann 2009 - Screening Panels For Detection of Monoclonal GammopathiesDokument6 SeitenKatzmann 2009 - Screening Panels For Detection of Monoclonal GammopathiesELISANoch keine Bewertungen
- Multiple Myeloma in IndonesiaDokument6 SeitenMultiple Myeloma in IndonesiaAnctho LukmiNoch keine Bewertungen