Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- ATLS Examination Questions and Answers 2019Dokument4 SeitenATLS Examination Questions and Answers 2019Kamalan Push25% (8)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Nursing Care Plan Urinary Tract Infection (UTI)Dokument2 SeitenNursing Care Plan Urinary Tract Infection (UTI)deric95% (97)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Maternal DistressDokument7 SeitenMaternal DistressBharat Thapa83% (6)
- Ewing's SarcomaDokument16 SeitenEwing's SarcomaChacha Zakiya100% (1)
- AIA Guidelines For HospitalsDokument100 SeitenAIA Guidelines For Hospitalsdrabhi23100% (18)
- AIA Guidelines For HospitalsDokument100 SeitenAIA Guidelines For Hospitalsdrabhi23100% (18)
- Engaging Physicians in A Shared Quality Agenda: Innovation Series 2007Dokument52 SeitenEngaging Physicians in A Shared Quality Agenda: Innovation Series 2007drabhi23Noch keine Bewertungen
- WHO Guidelines - Adverse EventsDokument80 SeitenWHO Guidelines - Adverse Eventsdrabhi23Noch keine Bewertungen
- MHA Strategic ManagementDokument87 SeitenMHA Strategic Managementdrabhi23Noch keine Bewertungen
- CP Compliance ToolDokument1 SeiteCP Compliance Tooldrabhi23Noch keine Bewertungen
- MHA Strategic ManagementDokument87 SeitenMHA Strategic Managementdrabhi23Noch keine Bewertungen
- Universal Precaution WhoDokument2 SeitenUniversal Precaution WhoYayu PujiNoch keine Bewertungen
- Family MedicineDokument1 SeiteFamily Medicinedrabhi23Noch keine Bewertungen
- Tumor Markers in Clinical Practice: General Principles and GuidelinesDokument8 SeitenTumor Markers in Clinical Practice: General Principles and GuidelinesNurmalia SariNoch keine Bewertungen
- NCPDokument8 SeitenNCPzharienabNoch keine Bewertungen
- Mayo Clinic Bells PalsyDokument4 SeitenMayo Clinic Bells PalsyCS NarayananNoch keine Bewertungen
- Incompetent Cervix As One of The Antenatal ComplicationsDokument14 SeitenIncompetent Cervix As One of The Antenatal ComplicationsKenje Kate Agripo100% (2)
- Licorice Root - Benefits, Uses, Precautions, and DosageDokument16 SeitenLicorice Root - Benefits, Uses, Precautions, and DosageSUMITNoch keine Bewertungen
- NSTP - Health AwarenessDokument21 SeitenNSTP - Health AwarenessAvril SalenNoch keine Bewertungen
- Increased Intracranial Pressure (IICP)Dokument2 SeitenIncreased Intracranial Pressure (IICP)Giselle Chloe Baluya icoNoch keine Bewertungen
- Hypertension CaseDokument3 SeitenHypertension CaseArnold Christian QuilonNoch keine Bewertungen
- Sideroblastic Anemia-: - Anemia in Which Bone Marrow Produces Ringed Sideroblasts Rather Than Healthy Red Blood Cells.Dokument31 SeitenSideroblastic Anemia-: - Anemia in Which Bone Marrow Produces Ringed Sideroblasts Rather Than Healthy Red Blood Cells.Suganya SelvamNoch keine Bewertungen
- Care Plan Prep May 13 Rheumatic FeverDokument16 SeitenCare Plan Prep May 13 Rheumatic Feverapi-256360167Noch keine Bewertungen
- Chapter 69Dokument47 SeitenChapter 69Benjamin SchauerteNoch keine Bewertungen
- 4creatine and Diabetes - Supplements and NutritionDokument4 Seiten4creatine and Diabetes - Supplements and NutritionjesseNoch keine Bewertungen
- Nasopharyngeal CarcinomaDokument25 SeitenNasopharyngeal Carcinomananda surastyo100% (1)
- 25 Myomectomy Consent FormDokument4 Seiten25 Myomectomy Consent FormDrscottmccallNoch keine Bewertungen
- Basic Cut Razor Sharp AbsDokument12 SeitenBasic Cut Razor Sharp AbsHelboy BautistaNoch keine Bewertungen
- Menieres DiseaseDokument6 SeitenMenieres Diseasecceng06Noch keine Bewertungen
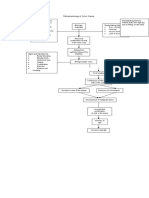
- Pathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorsDokument1 SeitePathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorstatiNoch keine Bewertungen
- Non Operative Treatment OA MadiunDokument46 SeitenNon Operative Treatment OA Madiunagus susantoNoch keine Bewertungen
- LRP VGFDPI 2021 004 - ProtocolDokument25 SeitenLRP VGFDPI 2021 004 - ProtocolDileep CRCNoch keine Bewertungen
- Radiotherapy and Oncology: Perioperative Management of SarcomaDokument8 SeitenRadiotherapy and Oncology: Perioperative Management of SarcomaNevine HannaNoch keine Bewertungen
- ECG and ArrhythmiasDokument25 SeitenECG and ArrhythmiasRashed ShatnawiNoch keine Bewertungen
- Small Bowel Obstruction: Bondoc, John Benedict V. FEU-NRMF Clinical Clerk M18Dokument24 SeitenSmall Bowel Obstruction: Bondoc, John Benedict V. FEU-NRMF Clinical Clerk M18John Benedict BondocNoch keine Bewertungen
- QR HypertensionDokument8 SeitenQR Hypertensionwaniaqilah workNoch keine Bewertungen
- Uterine AtonyDokument4 SeitenUterine AtonyThirdie LacorteNoch keine Bewertungen
- Postural DrainageDokument25 SeitenPostural DrainageMarivic DianoNoch keine Bewertungen
- Ledderhose Disease: Pathophysiology Diagnosis and ManagementDokument3 SeitenLedderhose Disease: Pathophysiology Diagnosis and ManagementLeandro PolancoNoch keine Bewertungen