Das könnte Ihnen auch gefallen
- Mechanical Ventilation 8.2.17Dokument41 SeitenMechanical Ventilation 8.2.17SyafiqAziziNoch keine Bewertungen
- Z Track Injection TechniqueDokument3 SeitenZ Track Injection TechniquebunsokoyNoch keine Bewertungen
- DialysisDokument4 SeitenDialysisClarise Ann GubatanNoch keine Bewertungen
- Nasogastric Tube Feeding ML3522Dokument5 SeitenNasogastric Tube Feeding ML3522Anonymous 0gUash0BxNoch keine Bewertungen
- Caring For A Gastrostomy TubeDokument13 SeitenCaring For A Gastrostomy TubeBianca DizonNoch keine Bewertungen
- Inserting A Nasogastric Tube (Checklist)Dokument13 SeitenInserting A Nasogastric Tube (Checklist)Mari Sheanne M. VasquezNoch keine Bewertungen
- Lower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDokument95 SeitenLower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingRI NANoch keine Bewertungen
- Cardiac EmergenciesDokument38 SeitenCardiac Emergenciesnurasia oktianiNoch keine Bewertungen
- By Abayneh Ayele (Ieso Student) Wollo UniversityDokument68 SeitenBy Abayneh Ayele (Ieso Student) Wollo UniversitydenekeNoch keine Bewertungen
- Acute Pyelonephritis Treatment & Management: Approach ConsiderationsDokument4 SeitenAcute Pyelonephritis Treatment & Management: Approach ConsiderationsPeter InocandoNoch keine Bewertungen
- Asthma and CopdDokument44 SeitenAsthma and CopdBeer Dilacshe100% (1)
- Suctioning TracheaDokument24 SeitenSuctioning Trachealuis_chubee100% (1)
- Chronic Renal Failure enDokument2 SeitenChronic Renal Failure enSinggih Pratiknyo SundawaNoch keine Bewertungen
- Heart Blood HistoDokument53 SeitenHeart Blood HistoAnonymous 52lBinNoch keine Bewertungen
- Oxygen Therapy: By: Melanie S. Cambel, MAN RNDokument21 SeitenOxygen Therapy: By: Melanie S. Cambel, MAN RNGeraldine MaeNoch keine Bewertungen
- How Bloodis Propelled Throughthe Hum An Ci Rcula To Ry Sy StemDokument5 SeitenHow Bloodis Propelled Throughthe Hum An Ci Rcula To Ry Sy Stemridwan100% (1)
- OxygenationDokument57 SeitenOxygenationassumptaNoch keine Bewertungen
- Suctioning Artificial Airways - AdultsDokument27 SeitenSuctioning Artificial Airways - AdultssdaNoch keine Bewertungen
- ARDS Care Respiratory Care Plan PDFDokument2 SeitenARDS Care Respiratory Care Plan PDFeric parlNoch keine Bewertungen
- Heart CareDokument14 SeitenHeart CareArman CareNoch keine Bewertungen
- Principles of Blood Transfusion 2Dokument21 SeitenPrinciples of Blood Transfusion 2dhivya singhNoch keine Bewertungen
- Essential Hypertension ManagementDokument5 SeitenEssential Hypertension Managementspicychips7Noch keine Bewertungen
- ASTHMADokument48 SeitenASTHMAifcrstarsNoch keine Bewertungen
- 2022 Pulse Oximetry and CapnographyDokument33 Seiten2022 Pulse Oximetry and CapnographyMohmmed MousaNoch keine Bewertungen
- IV Solutions CheatsheetDokument1 SeiteIV Solutions CheatsheetRevNoch keine Bewertungen
- Renal FailureDokument11 SeitenRenal FailureLindsey MeimbanNoch keine Bewertungen
- Cardiogenic Shock: Sparsh Goel 77Dokument28 SeitenCardiogenic Shock: Sparsh Goel 77Sparsh GoelNoch keine Bewertungen
- Acute Limb Ischemia - WucDokument37 SeitenAcute Limb Ischemia - WucOTOH RAYA OMARNoch keine Bewertungen
- Chest Injuries: DR Rodwell Gundo Medical/Surgical Nursing DepartmentDokument47 SeitenChest Injuries: DR Rodwell Gundo Medical/Surgical Nursing Departmentpaul kaundaNoch keine Bewertungen
- Seminar Asthma PDFDokument39 SeitenSeminar Asthma PDFAriff Mahdzub0% (1)
- Inserting A Nasogastric TubeDokument5 SeitenInserting A Nasogastric TubeWendy EscalanteNoch keine Bewertungen
- Drugs Affecting Renal FunctionDokument47 SeitenDrugs Affecting Renal FunctionMuhammad Shahid BilalNoch keine Bewertungen
- CABGDokument6 SeitenCABGBess RompalNoch keine Bewertungen
- DefibrillationDokument9 SeitenDefibrillationJara Maris Moreno BudionganNoch keine Bewertungen
- History of NursingDokument105 SeitenHistory of NursingHeide Basing-aNoch keine Bewertungen
- Types of PneumoniaDokument6 SeitenTypes of PneumoniasakuraleeshaoranNoch keine Bewertungen
- Cardiovascular SytemDokument56 SeitenCardiovascular SytemlindapramusintaNoch keine Bewertungen
- Airway ManagementDokument13 SeitenAirway ManagementAlaa DaoudNoch keine Bewertungen
- MNT in Diseases of Kidney and UrinaryDokument38 SeitenMNT in Diseases of Kidney and UrinaryJosephine A. Bertulfo100% (1)
- Poisoning DecontaminationDokument14 SeitenPoisoning DecontaminationadystiNoch keine Bewertungen
- Endocrine EmergenciesDokument52 SeitenEndocrine EmergenciesAdi ParamarthaNoch keine Bewertungen
- Cardiac ArrestDokument54 SeitenCardiac ArrestIdha FitriyaniNoch keine Bewertungen
- Pneumonia: DefinitionDokument5 SeitenPneumonia: DefinitionhemaanandhyNoch keine Bewertungen
- Head To Toe ExaminationDokument6 SeitenHead To Toe ExaminationFadillah Raisyah MNoch keine Bewertungen
- Abdominal IncisionDokument4 SeitenAbdominal IncisionMohit KumarNoch keine Bewertungen
- Specimen Collection, Transport and ProcessingDokument29 SeitenSpecimen Collection, Transport and ProcessingGladys Marie WillkomNoch keine Bewertungen
- Thoracic Trauma: Kenyatta University LectureDokument25 SeitenThoracic Trauma: Kenyatta University LectureIrene Zae MwandotoNoch keine Bewertungen
- Shock and SIRSDokument85 SeitenShock and SIRSBryan Mae H. DegorioNoch keine Bewertungen
- Preoperative Preparation of Patient For SurgeryDokument23 SeitenPreoperative Preparation of Patient For SurgeryFauzi SebunyaNoch keine Bewertungen
- Nursing Management of Mechanically Ventilated PatientsDokument179 SeitenNursing Management of Mechanically Ventilated PatientsSourabh AlawaNoch keine Bewertungen
- Diagnostic Procedures in Respiratory DiseaseDokument41 SeitenDiagnostic Procedures in Respiratory DiseaseVio Mincu50% (2)
- Thrombolytic TherapyDokument9 SeitenThrombolytic Therapymedic99Noch keine Bewertungen
- Pharmacology Assignment No.02: Submitted By: Submitted To: Nandraj Ma'am Areeba Shafiq Roll No. 1817007Dokument23 SeitenPharmacology Assignment No.02: Submitted By: Submitted To: Nandraj Ma'am Areeba Shafiq Roll No. 1817007Nandraj123100% (1)
- Respiratory DiseasesDokument11 SeitenRespiratory DiseasesMichael Angelo SeñaNoch keine Bewertungen
- Splints and Tractions in OrthopaedicsDokument56 SeitenSplints and Tractions in OrthopaedicsNinaNoch keine Bewertungen
- Antiarrhythmic Drugs by ZebDokument40 SeitenAntiarrhythmic Drugs by ZebFazl UllahNoch keine Bewertungen
- Cyanotic Congenital Heart DiseasesDokument25 SeitenCyanotic Congenital Heart DiseasesAlvin OmondiNoch keine Bewertungen
- ECG Made EasyDokument82 SeitenECG Made EasyBobby SodhiNoch keine Bewertungen
- Mechanical Ventilation - ModesDokument40 SeitenMechanical Ventilation - ModesabdallahNoch keine Bewertungen
- Trust Guideline For Neonatal Volume Guarantee Ventilation (VGV)Dokument8 SeitenTrust Guideline For Neonatal Volume Guarantee Ventilation (VGV)mohamedkorieshNoch keine Bewertungen
- Nursing Pocket Card - Mechanical Ventilation Settings and Basic Modes - June 2020 PDFDokument6 SeitenNursing Pocket Card - Mechanical Ventilation Settings and Basic Modes - June 2020 PDFmohamedkorieshNoch keine Bewertungen
- Increased RR Rate: Ensure All Alarms Are Set With Appropriate Parameters Each Shift!Dokument1 SeiteIncreased RR Rate: Ensure All Alarms Are Set With Appropriate Parameters Each Shift!mohamedkorieshNoch keine Bewertungen
- Settings and Management Tip Sheet For Providers: Isp Elevated?Dokument1 SeiteSettings and Management Tip Sheet For Providers: Isp Elevated?mohamedkorieshNoch keine Bewertungen
- Respiratory Therapy Pocket Reference: Ifnopt TriggerDokument2 SeitenRespiratory Therapy Pocket Reference: Ifnopt TriggermohamedkorieshNoch keine Bewertungen
- Dse5510 Installation InstDokument2 SeitenDse5510 Installation Instricardo_dionisi2700Noch keine Bewertungen
- HHW 35 m6 GBDokument6 SeitenHHW 35 m6 GBSuper WhippedNoch keine Bewertungen
- OK Flux 231 (F7AZ-EL12) PDFDokument2 SeitenOK Flux 231 (F7AZ-EL12) PDFborovniskiNoch keine Bewertungen
- Saurabh ShrivastavaDokument37 SeitenSaurabh ShrivastavaMahendraNoch keine Bewertungen
- SFF 8448Dokument8 SeitenSFF 8448eleptonNoch keine Bewertungen
- Pavement Evaluation and Overlay Des - DR MSA - LatestDokument103 SeitenPavement Evaluation and Overlay Des - DR MSA - LatestSreedhar BhuduruNoch keine Bewertungen
- Kalzip - Vapour Layer FR 0822 PDFDokument2 SeitenKalzip - Vapour Layer FR 0822 PDFBerat CakmakliNoch keine Bewertungen
- 006R5-WMS-JI-MI-MAU-ACS-II-23 Working Method - Pile CapDokument20 Seiten006R5-WMS-JI-MI-MAU-ACS-II-23 Working Method - Pile CapEko Budi HartantoNoch keine Bewertungen
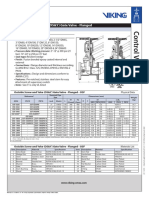
- Outside Screw and Yoke (OS&Y) Gate Valve - Flanged: Technical FeaturesDokument2 SeitenOutside Screw and Yoke (OS&Y) Gate Valve - Flanged: Technical FeaturesMark Louie GuintoNoch keine Bewertungen
- People Soft Bundle Release Note 9 Bundle9Dokument29 SeitenPeople Soft Bundle Release Note 9 Bundle9rajiv_xguysNoch keine Bewertungen
- Lecture 1 - Intro and SolidWorks PCBDokument17 SeitenLecture 1 - Intro and SolidWorks PCBmyturtle gameNoch keine Bewertungen
- T.C. Electronic M3000 User ManualDokument78 SeitenT.C. Electronic M3000 User ManualStanleyNoch keine Bewertungen
- Chapter.8: Oscillators: ObjectivesDokument13 SeitenChapter.8: Oscillators: ObjectivessivasankarnaiduNoch keine Bewertungen
- EWF2703 TV EmersonDokument57 SeitenEWF2703 TV EmersonEriksson Miguel Tapia SolisNoch keine Bewertungen
- FD100 CatalogoDokument4 SeitenFD100 CatalogoKaren VásconezNoch keine Bewertungen
- FlowCon FAC6HP Instruction 04 2013Dokument4 SeitenFlowCon FAC6HP Instruction 04 2013Jeff Anderson CollinsNoch keine Bewertungen
- Parts Catalog: Paper Feed Unit Type 3800C (G568)Dokument23 SeitenParts Catalog: Paper Feed Unit Type 3800C (G568)poldisagtNoch keine Bewertungen
- 16PPE723Dokument2 Seiten16PPE723DrArun KaliappanNoch keine Bewertungen
- Use of Multimeter TextDokument76 SeitenUse of Multimeter Textprueba1100% (2)
- One Pipe Steam DesignDokument44 SeitenOne Pipe Steam Designreyes hernandezNoch keine Bewertungen
- Subsea AccumulatorsDokument4 SeitenSubsea AccumulatorsAbdul Hameed OmarNoch keine Bewertungen
- Seismic Force CANADA Code - CNBC2005-V421Dokument7 SeitenSeismic Force CANADA Code - CNBC2005-V421Niko NištićNoch keine Bewertungen
- Flabeg Solar enDokument11 SeitenFlabeg Solar enZeec NoorNoch keine Bewertungen
- State of Patriot MissilesDokument13 SeitenState of Patriot MissilesTaira Mai100% (1)
- Stelzer Catalog PDFDokument12 SeitenStelzer Catalog PDFlhphong021191Noch keine Bewertungen
- Kohler 14 20 RES Parts Manual TP 6806 2016 06Dokument76 SeitenKohler 14 20 RES Parts Manual TP 6806 2016 06peleniusNoch keine Bewertungen
- Material Test Report: ISO EN 10204 2004-3.1Dokument4 SeitenMaterial Test Report: ISO EN 10204 2004-3.1Johan Sebastian C. SNoch keine Bewertungen
- Project Title: Hotel Management Software Project: PurposeDokument3 SeitenProject Title: Hotel Management Software Project: PurposesuryaNoch keine Bewertungen
- Liquid Gas Absorption ProcessDokument89 SeitenLiquid Gas Absorption ProcessMohd Masri A. RazakNoch keine Bewertungen
- Up-F-020 Solicitud de Admisión de Practicantes Ver-08Dokument108 SeitenUp-F-020 Solicitud de Admisión de Practicantes Ver-08MARCOS RODOLFO MALDONADO ZEVALLOSNoch keine Bewertungen