Das könnte Ihnen auch gefallen
- ELECTGROMAGNETIC SPECTRUM-RW TRANSMISSION & RECEPTION (Autosaved)Dokument17 SeitenELECTGROMAGNETIC SPECTRUM-RW TRANSMISSION & RECEPTION (Autosaved)Melai Rodriguez Ibardaloza73% (11)
- Earth Science PDFDokument371 SeitenEarth Science PDFSherlice Rom - Belista50% (2)
- 10-Implementing Policies and ProceduresDokument56 Seiten10-Implementing Policies and ProceduresMelai Rodriguez IbardalozaNoch keine Bewertungen
- Holistic Health Therapies For Cancer Barbara Clear BridgeDokument49 SeitenHolistic Health Therapies For Cancer Barbara Clear BridgetorontonianoNoch keine Bewertungen
- The COAT & Review Approach: How to recognise and manage unwell patientsVon EverandThe COAT & Review Approach: How to recognise and manage unwell patientsBewertung: 5 von 5 Sternen5/5 (1)
- Electromagnetism (Autosaved)Dokument45 SeitenElectromagnetism (Autosaved)Melai Rodriguez IbardalozaNoch keine Bewertungen
- KPI Discussion Paper 3Dokument22 SeitenKPI Discussion Paper 3Manager HR Hijaz Hospital100% (1)
- Quality Manager Job Description - 09-13Dokument3 SeitenQuality Manager Job Description - 09-13DrSaswat LincolnNoch keine Bewertungen
- Screw Retained Vs Cement Retained Implant-Supported Fixed Dental ProsthesisDokument11 SeitenScrew Retained Vs Cement Retained Implant-Supported Fixed Dental ProsthesisMario Troncoso AndersennNoch keine Bewertungen
- MODULE 3 STUDENT National Patient Safety Goals 2013Dokument15 SeitenMODULE 3 STUDENT National Patient Safety Goals 2013Dewi Ratna Sari100% (1)
- En - 2025-123-1837662383-Nursing KPI 2013 - FINALDokument9 SeitenEn - 2025-123-1837662383-Nursing KPI 2013 - FINALIamnurse NylejNoch keine Bewertungen
- IPSG PresentationDokument38 SeitenIPSG Presentationmuhammed shamaa100% (1)
- Strengthen Patient Experience: (Implementation Plan of IDC Program) Domain 3Dokument17 SeitenStrengthen Patient Experience: (Implementation Plan of IDC Program) Domain 3Rina LestariNoch keine Bewertungen
- JCI QUESTIONNAIRE-PCI Dept.Dokument6 SeitenJCI QUESTIONNAIRE-PCI Dept.Rabiya Sajjad100% (2)
- Dr. Lavanya - Infection Control Risk Assessment (ICRA)Dokument37 SeitenDr. Lavanya - Infection Control Risk Assessment (ICRA)Lucas TobingNoch keine Bewertungen
- Autoclave GuideDokument48 SeitenAutoclave GuideIman 111Noch keine Bewertungen
- 1nursing and Ethics.Dokument260 Seiten1nursing and Ethics.Emanuel Acray NkondolaNoch keine Bewertungen
- 0555 - Healthcare Risk Assessment Made Easy PDFDokument16 Seiten0555 - Healthcare Risk Assessment Made Easy PDFCecilia YeniNoch keine Bewertungen
- Annual Appraisal 2019 EDokument2 SeitenAnnual Appraisal 2019 EPrince Jhessie L. AbellaNoch keine Bewertungen
- Availability of Essential Supplies & EquipmentDokument2 SeitenAvailability of Essential Supplies & EquipmentLovelydePerioNoch keine Bewertungen
- 1.medication ErrorsDokument25 Seiten1.medication ErrorshussainNoch keine Bewertungen
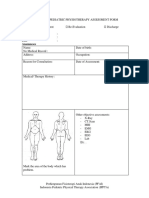
- Form PEMERIKSANAAN UMUM FT ANAK 300419Dokument4 SeitenForm PEMERIKSANAAN UMUM FT ANAK 300419vanoNoch keine Bewertungen
- Infection Prevention and Control Assessment Tool For Outpatient SettingsDokument22 SeitenInfection Prevention and Control Assessment Tool For Outpatient SettingsVera IndrawatiNoch keine Bewertungen
- JCI Standard Manual Guide For QM and Medical DirectorDokument1 SeiteJCI Standard Manual Guide For QM and Medical DirectorCyrene Diane Riego Roxas-ManzanoNoch keine Bewertungen
- Radiology ServicesDokument5 SeitenRadiology Servicesshah007zaadNoch keine Bewertungen
- Policies and ProceduresDokument24 SeitenPolicies and ProceduresAbdulazizNoch keine Bewertungen
- FMEA10 Sample PagesDokument24 SeitenFMEA10 Sample Pageswy1suwirjaNoch keine Bewertungen
- QA For Radiology DepartmentDokument3 SeitenQA For Radiology DepartmentRaviraj Pishe100% (1)
- Obeid Specialized Hospital - Riyadh: Quality Indicator Form 2018 2019Dokument2 SeitenObeid Specialized Hospital - Riyadh: Quality Indicator Form 2018 2019LovelydePerioNoch keine Bewertungen
- How To Identify and Analyze A Hospital Risk Assessment: Risk Management Part of The Higher PlanDokument12 SeitenHow To Identify and Analyze A Hospital Risk Assessment: Risk Management Part of The Higher Planver_at_workNoch keine Bewertungen
- Obeid Specialized Hospital - Riyadh: Key Performance Indiactors Second Quarter - 2019Dokument29 SeitenObeid Specialized Hospital - Riyadh: Key Performance Indiactors Second Quarter - 2019LovelydePerioNoch keine Bewertungen
- CBAHI IndicatorsDokument4 SeitenCBAHI IndicatorsJery Js0% (1)
- 2018 JCI Sentinel - Event - Policy1 PDFDokument5 Seiten2018 JCI Sentinel - Event - Policy1 PDFAhmedNoch keine Bewertungen
- Challenges For AccreditationDokument22 SeitenChallenges For AccreditationMohammad Muntaz AliNoch keine Bewertungen
- Nursing InformaticsDokument28 SeitenNursing Informaticsd1choosenNoch keine Bewertungen
- Quality Introduction: Performance IndicatorDokument28 SeitenQuality Introduction: Performance IndicatorLiza VarouqaNoch keine Bewertungen
- Annex G - Infection Control Annual Plan 2012-13Dokument7 SeitenAnnex G - Infection Control Annual Plan 2012-13Tianti PuadiNoch keine Bewertungen
- JCI Accreditation in The Operating Room Hospital Infection Prevention and Control of The Implementation of Standards and Experience ofDokument3 SeitenJCI Accreditation in The Operating Room Hospital Infection Prevention and Control of The Implementation of Standards and Experience ofMohamed FouadNoch keine Bewertungen
- Emergency NursingDokument15 SeitenEmergency NursingAshley Ishika100% (1)
- Scripps Hospital Patient Visitor Policy PDFDokument2 SeitenScripps Hospital Patient Visitor Policy PDFcode4saleNoch keine Bewertungen
- Joint Commission International: Nepomuceno, Rose Ann TDokument42 SeitenJoint Commission International: Nepomuceno, Rose Ann TRoan Nepomuceno - Joaquin100% (1)
- Ampullary Carcinoma: Treatment and PrognosisDokument24 SeitenAmpullary Carcinoma: Treatment and PrognosisHugo Alves100% (1)
- Hiv Consent Form PDFDokument2 SeitenHiv Consent Form PDFArka Prava PaulNoch keine Bewertungen
- Annual Report of Durdans HospitalDokument176 SeitenAnnual Report of Durdans HospitaloshanNoch keine Bewertungen
- Annual Infection Control Report Für 2021Dokument26 SeitenAnnual Infection Control Report Für 2021Ruby Joyce AguilarNoch keine Bewertungen
- Infection Control NHS PolicyDokument12 SeitenInfection Control NHS PolicyYahya Salem100% (1)
- Mpp-Verification of Prescription OrdersDokument6 SeitenMpp-Verification of Prescription OrdersMelai Rodriguez IbardalozaNoch keine Bewertungen
- JCI International Library of Measures ANIK BUKUDokument325 SeitenJCI International Library of Measures ANIK BUKUnurulNoch keine Bewertungen
- MED. Dental Services (Infection Control 2) .002docDokument8 SeitenMED. Dental Services (Infection Control 2) .002docKenny JosefNoch keine Bewertungen
- CBAhi-Quality Management & Patient SafetyDokument14 SeitenCBAhi-Quality Management & Patient SafetyJery JsNoch keine Bewertungen
- Brenda Creaney PresentationDokument21 SeitenBrenda Creaney Presentationmonir61Noch keine Bewertungen
- Daftar Panduan JCIDokument12 SeitenDaftar Panduan JCIEko Wahyu AgustinNoch keine Bewertungen
- Sentinel Events: Vidya PrasadDokument21 SeitenSentinel Events: Vidya PrasadTOUSHIFAHEMEDNoch keine Bewertungen
- A P Policy & Procedure: Ntibiotic OlicyDokument24 SeitenA P Policy & Procedure: Ntibiotic Olicyvijay kumarNoch keine Bewertungen
- 2007 International Patient Safety GoalsDokument1 Seite2007 International Patient Safety GoalsElias Baraket FreijyNoch keine Bewertungen
- Safety Event Reporting PolicyDokument10 SeitenSafety Event Reporting PolicypatientsafetyNoch keine Bewertungen
- Nhs 3rd Edition V 1.1 - CbahiDokument2 SeitenNhs 3rd Edition V 1.1 - Cbahimohammad hamdanNoch keine Bewertungen
- Seminar JCI - 9 Feb 2012Dokument16 SeitenSeminar JCI - 9 Feb 2012Mahardika PertiwiNoch keine Bewertungen
- Implementation Guidelines For The Canadian Emergency Department Triage & Acuity Scale (CTAS)Dokument27 SeitenImplementation Guidelines For The Canadian Emergency Department Triage & Acuity Scale (CTAS)Jery JsNoch keine Bewertungen
- Quality AssuranceDokument43 SeitenQuality Assurancekanika100% (1)
- Civil Hospital Karachi Emergency PlanDokument25 SeitenCivil Hospital Karachi Emergency Plandr_bhuttoNoch keine Bewertungen
- Strategies To Improve Handoff CommunicationDokument2 SeitenStrategies To Improve Handoff CommunicationJames SimmonsNoch keine Bewertungen
- Homoeopathy Indicators NABHDokument105 SeitenHomoeopathy Indicators NABHMamoni MaityNoch keine Bewertungen
- ID FOI Patient Safety Learning Event Policy 20200421Dokument21 SeitenID FOI Patient Safety Learning Event Policy 20200421patientsafety100% (1)
- CHECKLIST - Crash Cart Policy and Checklist in HospitalDokument4 SeitenCHECKLIST - Crash Cart Policy and Checklist in HospitalSanjay KadamNoch keine Bewertungen
- RMO Assessment Form 2016Dokument8 SeitenRMO Assessment Form 2016Tp HoangNoch keine Bewertungen
- Presentation Q06 Certified ProfeDokument304 SeitenPresentation Q06 Certified ProfeMemo MedoNoch keine Bewertungen
- Principles of Oncology and Outline of ManagementDokument78 SeitenPrinciples of Oncology and Outline of ManagementPavan JonnadaNoch keine Bewertungen
- Patient Safety: What Should We Be Trying To Communicate?Dokument32 SeitenPatient Safety: What Should We Be Trying To Communicate?cicaklomenNoch keine Bewertungen
- Patient Safety Organization A Complete Guide - 2020 EditionVon EverandPatient Safety Organization A Complete Guide - 2020 EditionNoch keine Bewertungen
- Healthcare Environmental Services A Complete Guide - 2020 EditionVon EverandHealthcare Environmental Services A Complete Guide - 2020 EditionNoch keine Bewertungen
- Choir ATTENDANCEDokument4 SeitenChoir ATTENDANCEMelai Rodriguez IbardalozaNoch keine Bewertungen
- Electgromagnetic Spectrum-Radio WavesDokument10 SeitenElectgromagnetic Spectrum-Radio WavesMelai Rodriguez IbardalozaNoch keine Bewertungen
- Characteristics of EarthDokument13 SeitenCharacteristics of EarthMelai Rodriguez IbardalozaNoch keine Bewertungen
- Common Rock-Forming Minerals and Their Physical and Chemical PropertiesDokument15 SeitenCommon Rock-Forming Minerals and Their Physical and Chemical PropertiesMelai Rodriguez IbardalozaNoch keine Bewertungen
- ZipGrade50QuestionV2 PDFDokument1 SeiteZipGrade50QuestionV2 PDFMelai Rodriguez IbardalozaNoch keine Bewertungen
- Assessment of Learning OutcomesDokument52 SeitenAssessment of Learning OutcomesMelai Rodriguez IbardalozaNoch keine Bewertungen
- Table of Specifications Third Quarter Examination Mathematics 10Dokument1 SeiteTable of Specifications Third Quarter Examination Mathematics 10Melai Rodriguez IbardalozaNoch keine Bewertungen
- 1st Quarter Ovr, 1434Dokument14 Seiten1st Quarter Ovr, 1434Melai Rodriguez IbardalozaNoch keine Bewertungen
- Adverse Drug Reaction ReportDokument2 SeitenAdverse Drug Reaction ReportMelai Rodriguez IbardalozaNoch keine Bewertungen
- NARCOTIC&CONTROLLEDDokument56 SeitenNARCOTIC&CONTROLLEDMelai Rodriguez IbardalozaNoch keine Bewertungen
- Capitol University Medical Center PoliciesDokument5 SeitenCapitol University Medical Center PoliciesCharles CagaananNoch keine Bewertungen
- NCP Seizure FinalDokument4 SeitenNCP Seizure FinalLyrechel de GuzmanNoch keine Bewertungen
- 2009 Schedule of ExamDokument2 Seiten2009 Schedule of ExamPRC Baguio100% (13)
- IRMERDokument14 SeitenIRMERDr DoomNoch keine Bewertungen
- Multi-Disease Prediction Using Machine Learning AlgorithmDokument9 SeitenMulti-Disease Prediction Using Machine Learning AlgorithmIJRASETPublicationsNoch keine Bewertungen
- Let's Talk About New Jobs : AnswersDokument3 SeitenLet's Talk About New Jobs : AnswersosmarNoch keine Bewertungen
- Title:-Iot Based Health Monitoring System Using Raspberry PiDokument28 SeitenTitle:-Iot Based Health Monitoring System Using Raspberry PiGagan DeepNoch keine Bewertungen
- Ati - RN Comprehensive Predictor 2023 RemediationDokument21 SeitenAti - RN Comprehensive Predictor 2023 Remediationseansdrew2Noch keine Bewertungen
- Health Sector EHSMS - 9!12!2015Dokument35 SeitenHealth Sector EHSMS - 9!12!2015YL LYNoch keine Bewertungen
- Inhouse TPA - Claim FormDokument2 SeitenInhouse TPA - Claim FormJanarthanan KNoch keine Bewertungen
- Comfort Measures: A Concept Analysis: Irene Oliveira, RN, BSCNDokument21 SeitenComfort Measures: A Concept Analysis: Irene Oliveira, RN, BSCNLina Mahayaty SembiringNoch keine Bewertungen
- Analytical Study To Understand The Role of Homoeopathic Medicines in Patients Suffering From The Complaint of Back PainDokument3 SeitenAnalytical Study To Understand The Role of Homoeopathic Medicines in Patients Suffering From The Complaint of Back PainEditor IJTSRDNoch keine Bewertungen
- Max Medic Plan 1Dokument1 SeiteMax Medic Plan 1Premkumar NadarajanNoch keine Bewertungen
- 2019 Spena and Cristina Practising Innovation in The Healthcare EcosystemDokument14 Seiten2019 Spena and Cristina Practising Innovation in The Healthcare Ecosystemwihaga satya khresnaNoch keine Bewertungen
- Prevention ObesityDokument13 SeitenPrevention ObesityDaira QuinteroNoch keine Bewertungen
- Doctor X.ep01.480p.x264 (D Addicts)Dokument54 SeitenDoctor X.ep01.480p.x264 (D Addicts)an006Noch keine Bewertungen
- Askep Demensia GerontikDokument8 SeitenAskep Demensia Gerontikjoveny meining tyas0% (1)
- Case Session - 5Dokument3 SeitenCase Session - 5Ruthwick GowdaNoch keine Bewertungen
- November: Editor in Chief Managing Editor Coordinator ContributorsDokument7 SeitenNovember: Editor in Chief Managing Editor Coordinator ContributorsdeltawomenNoch keine Bewertungen
- TL3 8 Garbim2021Dokument33 SeitenTL3 8 Garbim2021bomonnhacongdongNoch keine Bewertungen
- Satera Gause Annotated BibDokument3 SeitenSatera Gause Annotated Bibapi-264107234Noch keine Bewertungen
- BSRTDokument1 SeiteBSRTPaul John HipolitoNoch keine Bewertungen
- Smart PumpsDokument98 SeitenSmart PumpsVictor Akira Santos SatoNoch keine Bewertungen