Das könnte Ihnen auch gefallen
- MED 1.4 PE of The Chest, Lungs, Breast, and Axilla PDFDokument16 SeitenMED 1.4 PE of The Chest, Lungs, Breast, and Axilla PDFelleinasNoch keine Bewertungen
- Respiratory gymnastics (Translated): Purification - Health - Strength - EnergyVon EverandRespiratory gymnastics (Translated): Purification - Health - Strength - EnergyNoch keine Bewertungen
- Health Assessment Chapter 7 Assessment of Respiratory SystemDokument20 SeitenHealth Assessment Chapter 7 Assessment of Respiratory SystemnadyaNoch keine Bewertungen
- Draft JV Agreement (La Mesa Gardens Condominiums - Amparo Property)Dokument13 SeitenDraft JV Agreement (La Mesa Gardens Condominiums - Amparo Property)Patrick PenachosNoch keine Bewertungen
- Respiratory Examination: The Position of The PatientDokument24 SeitenRespiratory Examination: The Position of The PatientMuhammed Barznji100% (1)
- Assessment of Respiratory SystemDokument18 SeitenAssessment of Respiratory SystemIbi Yulia Setyani100% (1)
- Unit 06 Assessment of Thorax and LungDokument55 SeitenUnit 06 Assessment of Thorax and Lunghuma100% (1)
- Respiratory AssessmentDokument79 SeitenRespiratory AssessmentKarlo ReyesNoch keine Bewertungen
- Account Statement 250820 240920 PDFDokument2 SeitenAccount Statement 250820 240920 PDFUnknown100% (1)
- Thorax and The LungsDokument30 SeitenThorax and The Lungschifunndo charles100% (1)
- Data StructuresDokument4 SeitenData StructuresBenjB1983Noch keine Bewertungen
- Physical Diagnoses: Respiratory SystemDokument72 SeitenPhysical Diagnoses: Respiratory SystemAmanuel MaruNoch keine Bewertungen
- Pulmonary Assessment: Components of The AssessmentDokument7 SeitenPulmonary Assessment: Components of The Assessmentjoanna gurtizaNoch keine Bewertungen
- Assessment of Lung and ChestDokument50 SeitenAssessment of Lung and ChestAbdurehman Ayele100% (1)
- Pulmonary Assessment: Components of The AssessmentDokument6 SeitenPulmonary Assessment: Components of The AssessmentWenzy Razzie cruzNoch keine Bewertungen
- Hydraulic Mining ExcavatorDokument8 SeitenHydraulic Mining Excavatorasditia_07100% (1)
- Respiratory AssessmentDokument43 SeitenRespiratory AssessmentLui Andrei AnilaNoch keine Bewertungen
- Clinical Examination of Respiratory SystemDokument37 SeitenClinical Examination of Respiratory SystemDipienshu BhatNoch keine Bewertungen
- Respiratory Examination OSCE GuideDokument14 SeitenRespiratory Examination OSCE GuideSam James100% (1)
- Assessment of Respiratory SystemDokument34 SeitenAssessment of Respiratory SystemKristal Jade Yanto Esquillo100% (1)
- Care of A Child With RespiratoryDokument185 SeitenCare of A Child With RespiratoryVanessa Lopez100% (1)
- NIQS BESMM 4 BillDokument85 SeitenNIQS BESMM 4 BillAliNoch keine Bewertungen
- Examination of The Respiratory SystemDokument35 SeitenExamination of The Respiratory SystemRashhmi Karthodi100% (1)
- Assessing The Thorax and The LungsDokument9 SeitenAssessing The Thorax and The LungsChrizzia Del RosarioNoch keine Bewertungen
- CLG418 (Dcec) PM 201409022-EnDokument1.143 SeitenCLG418 (Dcec) PM 201409022-EnMauricio WijayaNoch keine Bewertungen
- Causes and Possible Prevention of Asthma and AllergiesVon EverandCauses and Possible Prevention of Asthma and AllergiesNoch keine Bewertungen
- Topic 1 - Pulmonary Anatomy, Physiology and Assessment (Hemo)Dokument39 SeitenTopic 1 - Pulmonary Anatomy, Physiology and Assessment (Hemo)Ben JilhanoNoch keine Bewertungen
- RSDokument12 SeitenRSKamalchandra NaikNoch keine Bewertungen
- Review NotesDokument9 SeitenReview NotesKhaskie Geneva DumaguinNoch keine Bewertungen
- Pemeriksaan Fisik Sistem Pernapasan: Equipment NeededDokument78 SeitenPemeriksaan Fisik Sistem Pernapasan: Equipment Neededsri karinaNoch keine Bewertungen
- Kuliah Pengantar PF ParuDokument62 SeitenKuliah Pengantar PF Parugagah152Noch keine Bewertungen
- Assessing The Thorax and The LungsDokument9 SeitenAssessing The Thorax and The LungsChrizzia Del RosarioNoch keine Bewertungen
- Assessment of Respiratory System PDFDokument41 SeitenAssessment of Respiratory System PDFsarhang talebaniNoch keine Bewertungen
- Respiratory System: Physical Diagnosis Course II Physical ExamDokument57 SeitenRespiratory System: Physical Diagnosis Course II Physical ExamashuNoch keine Bewertungen
- Lungs and ThoraxDokument9 SeitenLungs and ThoraxMaria Mika Ella RetizaNoch keine Bewertungen
- 14 Assessment of The Throax and LungDokument68 Seiten14 Assessment of The Throax and LungCruz YrNoch keine Bewertungen
- Basic Clinical SkillsDokument6 SeitenBasic Clinical SkillsBlake KamminNoch keine Bewertungen
- 5 - Respiratory AssessmentDokument61 Seiten5 - Respiratory AssessmentAbboud Ali100% (1)
- Respiratory System ExaminationDokument12 SeitenRespiratory System ExaminationHoussemNoch keine Bewertungen
- FU-M3-CU11 Respiratory Function and Nursing CareDokument17 SeitenFU-M3-CU11 Respiratory Function and Nursing CareHERLIN HOBAYANNoch keine Bewertungen
- Session 4 - Performing Respiratory System ExaminationDokument26 SeitenSession 4 - Performing Respiratory System ExaminationOtsward OwdenNoch keine Bewertungen
- CPAC SON HA 7 Thorax 1Dokument59 SeitenCPAC SON HA 7 Thorax 1misshalieediiNoch keine Bewertungen
- Objectives of Physical AssessmentDokument10 SeitenObjectives of Physical Assessmentemman_abz100% (1)
- Essential Parameters of Airway Evaluation Lecture 6Dokument27 SeitenEssential Parameters of Airway Evaluation Lecture 69yqgmkvyzdNoch keine Bewertungen
- DR Amsalu Bekele Ass - Professor of Medicine Head of Chest Unit Department of Internal Medicine Addis Ababa University, School of Medicine Addis Ababa, EthiopiaDokument81 SeitenDR Amsalu Bekele Ass - Professor of Medicine Head of Chest Unit Department of Internal Medicine Addis Ababa University, School of Medicine Addis Ababa, EthiopiaBethelhem BirhanuNoch keine Bewertungen
- Respiratory SystemDokument23 SeitenRespiratory SystemSaraNoch keine Bewertungen
- Resp AssessmentDokument19 SeitenResp AssessmentNURSES- NOOK & CORNERNoch keine Bewertungen
- Resp AssessmentDokument19 SeitenResp AssessmentNURSES- NOOK & CORNERNoch keine Bewertungen
- Respiratory System: Assessment: ObjectivesDokument19 SeitenRespiratory System: Assessment: ObjectivesNURSES- NOOK & CORNERNoch keine Bewertungen
- Oxygenation 1Dokument155 SeitenOxygenation 1Khatlen BagaresNoch keine Bewertungen
- 3 RespDokument81 Seiten3 RespashuNoch keine Bewertungen
- Lab Guide: Respiratory AssessmentDokument10 SeitenLab Guide: Respiratory AssessmentDaisy MellaNoch keine Bewertungen
- Pulmonary Examination - Knowledge at AMBOSSDokument1 SeitePulmonary Examination - Knowledge at AMBOSSKC Dela RosaNoch keine Bewertungen
- Lungs and Thorax Assessment - PPTX RAHEEM KHANDokument60 SeitenLungs and Thorax Assessment - PPTX RAHEEM KHANRabia IsrafilNoch keine Bewertungen
- Pemeriksaan ThoraxDokument27 SeitenPemeriksaan ThoraxYaasinta ArlaesNoch keine Bewertungen
- PalpationDokument44 SeitenPalpationjenyNoch keine Bewertungen
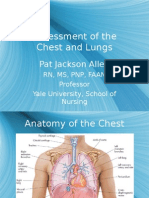
- Assessment of The Chest and Lungs: Pat Jackson AllenDokument50 SeitenAssessment of The Chest and Lungs: Pat Jackson Allenbuzz Q100% (3)
- Chest ExaminationDokument5 SeitenChest Examinationalin malekNoch keine Bewertungen
- Physical Exam - Chest 2006Dokument84 SeitenPhysical Exam - Chest 2006api-19916399Noch keine Bewertungen
- Physical Examination 2011Dokument171 SeitenPhysical Examination 2011Norakmal Andika YusriNoch keine Bewertungen
- Anatomy and Physiology of Respiratory SystemDokument6 SeitenAnatomy and Physiology of Respiratory SystemMonica VelascoNoch keine Bewertungen
- Lecture Respiratory Medicine - Clinical ExaminationDokument39 SeitenLecture Respiratory Medicine - Clinical Examinationgloria anyebeNoch keine Bewertungen
- Pemeriksaan ThoraxDokument27 SeitenPemeriksaan ThoraxSubchanPrasetyoNoch keine Bewertungen
- Advertising II Marathi VersionDokument91 SeitenAdvertising II Marathi VersionHarsh Sangani100% (1)
- Contoh Discussion Text Tentang HomeworkDokument8 SeitenContoh Discussion Text Tentang Homeworkg3p35rs6100% (1)
- LspciDokument4 SeitenLspciregistroosNoch keine Bewertungen
- Owners Manual Air Bike Unlimited Mag 402013Dokument28 SeitenOwners Manual Air Bike Unlimited Mag 402013David ChanNoch keine Bewertungen
- Measuring Temperature - Platinum Resistance ThermometersDokument3 SeitenMeasuring Temperature - Platinum Resistance Thermometersdark*nightNoch keine Bewertungen
- Brigade Product Catalogue Edition 20 EnglishDokument88 SeitenBrigade Product Catalogue Edition 20 EnglishPelotudoPeloteroNoch keine Bewertungen
- A Review of Service Quality ModelsDokument8 SeitenA Review of Service Quality ModelsJimmiJini100% (1)
- Open Source NetworkingDokument226 SeitenOpen Source NetworkingyemenlinuxNoch keine Bewertungen
- Frellwits Swedish Hosts FileDokument10 SeitenFrellwits Swedish Hosts FileAnonymous DsGzm0hQf5Noch keine Bewertungen
- Airport & Harbour Engg-AssignmentDokument3 SeitenAirport & Harbour Engg-AssignmentAshok Kumar RajanavarNoch keine Bewertungen
- Soil NailingDokument6 SeitenSoil Nailingvinodreddy146Noch keine Bewertungen
- Current Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiDokument8 SeitenCurrent Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiJoão Artur BonadimanNoch keine Bewertungen
- BJAS - Volume 5 - Issue Issue 1 Part (2) - Pages 275-281Dokument7 SeitenBJAS - Volume 5 - Issue Issue 1 Part (2) - Pages 275-281Vengky UtamiNoch keine Bewertungen
- Comparative Study Between Online and Offilne Learning With Reference of Tutedude E-LearningDokument61 SeitenComparative Study Between Online and Offilne Learning With Reference of Tutedude E-LearningDeeksha Saxena0% (2)
- Feed-Pump Hydraulic Performance and Design Improvement, Phase I: J2esearch Program DesignDokument201 SeitenFeed-Pump Hydraulic Performance and Design Improvement, Phase I: J2esearch Program DesignJonasNoch keine Bewertungen
- Assignment 4Dokument5 SeitenAssignment 4Hafiz AhmadNoch keine Bewertungen
- Binge Eating Disorder ANNADokument12 SeitenBinge Eating Disorder ANNAloloasbNoch keine Bewertungen
- WHO Guidelines For Drinking Water: Parameters Standard Limits As Per WHO Guidelines (MG/L)Dokument3 SeitenWHO Guidelines For Drinking Water: Parameters Standard Limits As Per WHO Guidelines (MG/L)114912Noch keine Bewertungen
- User Manual PM3250Dokument80 SeitenUser Manual PM3250otavioalcaldeNoch keine Bewertungen
- Mathematics BQP 2022Dokument43 SeitenMathematics BQP 2022muhammadmansuri815Noch keine Bewertungen
- TraceDokument5 SeitenTraceNorma TellezNoch keine Bewertungen
- Aakriti 1Dokument92 SeitenAakriti 1raghav bansalNoch keine Bewertungen
- TESTDokument27 SeitenTESTLegal CheekNoch keine Bewertungen
- A Medium-Rise Residential Building: A B C E D F G HDokument3 SeitenA Medium-Rise Residential Building: A B C E D F G HBabyjhaneTanItmanNoch keine Bewertungen