Das könnte Ihnen auch gefallen
- Theresa J. Llanes: ObjectiveDokument2 SeitenTheresa J. Llanes: Objectiveejg26Noch keine Bewertungen
- Chain of InfectionDokument2 SeitenChain of Infectionejg26Noch keine Bewertungen
- Honda Accord 95Dokument2 SeitenHonda Accord 95ejg26Noch keine Bewertungen
- Facebook or Facing Your BookDokument2 SeitenFacebook or Facing Your Bookejg26Noch keine Bewertungen
- Case StudyDokument2 SeitenCase Studyejg26Noch keine Bewertungen
- Freuds Psychosexual Stages of Development Oral StageDokument8 SeitenFreuds Psychosexual Stages of Development Oral Stageejg26Noch keine Bewertungen
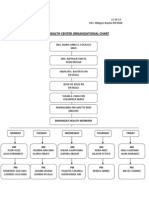
- Health Center: Organizational Chart Ampid 1 San Mateo, RizalDokument1 SeiteHealth Center: Organizational Chart Ampid 1 San Mateo, Rizalejg26Noch keine Bewertungen
- Purposes of SurgeryDokument2 SeitenPurposes of Surgeryejg26Noch keine Bewertungen
- Movie Reports DutyVLDokument9 SeitenMovie Reports DutyVLejg26Noch keine Bewertungen
- Dopa DobuDokument2 SeitenDopa Dobuejg26Noch keine Bewertungen
- Ketorolac Drug StudyDokument1 SeiteKetorolac Drug Studyejg26Noch keine Bewertungen
- Nursing Informatics in CanadaDokument25 SeitenNursing Informatics in Canadaejg26Noch keine Bewertungen
- Aaron Learning InsightsDokument1 SeiteAaron Learning Insightsejg26Noch keine Bewertungen
- Anti Tuberculosis AgentsDokument15 SeitenAnti Tuberculosis Agentsejg26100% (1)
- Rarejob Endorsement Letter For BpiDokument1 SeiteRarejob Endorsement Letter For Bpiejg26100% (2)
- Empire of The Sun Soc 18Dokument3 SeitenEmpire of The Sun Soc 18ejg26Noch keine Bewertungen
- QuizDokument2 SeitenQuizejg26Noch keine Bewertungen
- Roosevelt College System Institute of Nursing and Health Education Sumulong Highway Cainta, RizalDokument2 SeitenRoosevelt College System Institute of Nursing and Health Education Sumulong Highway Cainta, Rizalejg26Noch keine Bewertungen
- Report Sa Informatics!Dokument13 SeitenReport Sa Informatics!ejg26Noch keine Bewertungen
- Intake and Output Monitoring Sheet: Date TimeDokument3 SeitenIntake and Output Monitoring Sheet: Date Timeejg26Noch keine Bewertungen
- Roosevelt College System Institute of Nursing and Health Education Sumulong Highway Cainta, RizalDokument1 SeiteRoosevelt College System Institute of Nursing and Health Education Sumulong Highway Cainta, Rizalejg26Noch keine Bewertungen
- FNCP Health Center ChartDokument1 SeiteFNCP Health Center Chartejg26Noch keine Bewertungen
- FNCP Barangay ChartDokument1 SeiteFNCP Barangay Chartejg26Noch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Advantages and Disadvantages of Pareto AnalysisDokument3 SeitenAdvantages and Disadvantages of Pareto Analysisahmetganiozturk2Noch keine Bewertungen
- 11289Dokument15 Seiten11289medhaNoch keine Bewertungen
- Resume: House No. 1/2B, Delight Homes, Mob.-9696494900Dokument3 SeitenResume: House No. 1/2B, Delight Homes, Mob.-9696494900salmanNoch keine Bewertungen
- Nama: Ilma Adilla Syahida NIM: 04021281924030 Kelas Reguler A 2019 Psik FK Unsri ExerciseDokument3 SeitenNama: Ilma Adilla Syahida NIM: 04021281924030 Kelas Reguler A 2019 Psik FK Unsri Exerciseilma adilla syahidaNoch keine Bewertungen
- wsc2018 Schedule WebDokument46 Seitenwsc2018 Schedule WebAndrea AcriNoch keine Bewertungen
- AHMI Application For Enrolment - v11.2 Jan 2022Dokument11 SeitenAHMI Application For Enrolment - v11.2 Jan 2022Don MarquezNoch keine Bewertungen
- School To Prison PipelineDokument4 SeitenSchool To Prison Pipelineapi-253866947Noch keine Bewertungen
- Cambridge International Examinations Cambridge International General Certificate of Secondary EducationDokument20 SeitenCambridge International Examinations Cambridge International General Certificate of Secondary EducationequakeroatsNoch keine Bewertungen
- AbubakarDokument5 SeitenAbubakarJoshua MirandillaNoch keine Bewertungen
- Grade8 3RD Grading S1 S2 FinalDokument3 SeitenGrade8 3RD Grading S1 S2 FinalJanford BaculiNoch keine Bewertungen
- Moving To A New Country British English Student Ver2Dokument4 SeitenMoving To A New Country British English Student Ver2Paula LyrioNoch keine Bewertungen
- Memo On DreamersDokument3 SeitenMemo On DreamersAnonymous UFfj4cWO100% (8)
- Complete Mendel LessonDokument13 SeitenComplete Mendel Lessonapi-312176473Noch keine Bewertungen
- Reporter 563Dokument16 SeitenReporter 563gio477Noch keine Bewertungen
- Applied Social Psychology Understanding and Addressing Social and Practical Problems 3rd Edition Gruman Test BankDokument17 SeitenApplied Social Psychology Understanding and Addressing Social and Practical Problems 3rd Edition Gruman Test BankErin Gutierrez100% (34)
- Firo B-ParthDokument28 SeitenFiro B-ParthParth V. PurohitNoch keine Bewertungen
- Community Health Intervention ImplementationDokument3 SeitenCommunity Health Intervention ImplementationAudrey Ann AcobNoch keine Bewertungen
- Death Be Not Proud by John Gunther - Teacher Study GuideDokument1 SeiteDeath Be Not Proud by John Gunther - Teacher Study GuideHarperAcademicNoch keine Bewertungen
- Search Algorithms in Artificial IntelligenceDokument13 SeitenSearch Algorithms in Artificial IntelligencenandhiniNoch keine Bewertungen
- Developing A Business Simulation Game To Improve Student Engagement With Accounting TheoryDokument13 SeitenDeveloping A Business Simulation Game To Improve Student Engagement With Accounting TheoryIris DescentNoch keine Bewertungen
- Math Aisl t2 Ca1 QP - Grade 11Dokument9 SeitenMath Aisl t2 Ca1 QP - Grade 11hitarth shahNoch keine Bewertungen
- Accomplishment Report: EnrolmentDokument3 SeitenAccomplishment Report: EnrolmentShirney Naelga EscabarteNoch keine Bewertungen
- The Spread of BuddhismDokument484 SeitenThe Spread of BuddhismEdmund_Ding100% (2)
- Study On Training and Development of Construction CompanyDokument93 SeitenStudy On Training and Development of Construction CompanyAbhijeetNoch keine Bewertungen
- ML 1 2 3 4Dokument13 SeitenML 1 2 3 4satuNoch keine Bewertungen
- Diary of A Wimpy Kid (#1) - Jeff KinneyDokument142 SeitenDiary of A Wimpy Kid (#1) - Jeff KinneyDyan Anne Trompeta38% (13)
- Oop Manual 220173107016Dokument91 SeitenOop Manual 220173107016Kavish Panchal0% (1)
- Family Assessment ExampleDokument8 SeitenFamily Assessment Exampleim3in1100% (24)
- Past Present and Future of Swarm RoboticsDokument26 SeitenPast Present and Future of Swarm RoboticsJaishree SaraswatNoch keine Bewertungen
- Teacher Job Satisfaction Questionnaire (TJSQ) : Appendix FDokument4 SeitenTeacher Job Satisfaction Questionnaire (TJSQ) : Appendix FMohammed Demssie Mohammed100% (1)