Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Centor ScoreDokument8 SeitenCentor ScoreLoo DonNoch keine Bewertungen
- Post-Cardiac Arrest SyndromeDokument30 SeitenPost-Cardiac Arrest SyndromeAuliaRahmanNoch keine Bewertungen
- Chicken Pox Guidelines PDFDokument1 SeiteChicken Pox Guidelines PDFAuliaRahmanNoch keine Bewertungen
- Centor ScoreDokument8 SeitenCentor ScoreLoo DonNoch keine Bewertungen
- Anamnesis:: BB KG TB CM No - RM TGL - Masuk TGL - Lahir DPJPDokument4 SeitenAnamnesis:: BB KG TB CM No - RM TGL - Masuk TGL - Lahir DPJPAuliaRahmanNoch keine Bewertungen
- 10 1 1 563 4316 PDFDokument5 Seiten10 1 1 563 4316 PDFAuliaRahmanNoch keine Bewertungen
- Chicken Pox Guidelines PDFDokument1 SeiteChicken Pox Guidelines PDFAuliaRahmanNoch keine Bewertungen
- Jurnal OkeDokument8 SeitenJurnal OkeAuliaRahmanNoch keine Bewertungen
- Anamnesis:: BB KG TB CM No - RM TGL - Masuk TGL - Lahir DPJPDokument4 SeitenAnamnesis:: BB KG TB CM No - RM TGL - Masuk TGL - Lahir DPJPAuliaRahmanNoch keine Bewertungen
- RHDDokument130 SeitenRHDDeepu RajendranNoch keine Bewertungen
- Who TRS 923 PDFDokument130 SeitenWho TRS 923 PDFAuliaRahmanNoch keine Bewertungen
- Diagnosis of Childhood Acute Lymphoblastic Leukemia and Optimization of Risk-Benefit Ratio of TherapyDokument24 SeitenDiagnosis of Childhood Acute Lymphoblastic Leukemia and Optimization of Risk-Benefit Ratio of TherapyAuliaRahmanNoch keine Bewertungen
- 2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisDokument22 Seiten2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisAuliaRahmanNoch keine Bewertungen
- VACTERL-association EN PDFDokument12 SeitenVACTERL-association EN PDFAuliaRahmanNoch keine Bewertungen
- Makalah Brain GYM International, BDokument17 SeitenMakalah Brain GYM International, BAuliaRahmanNoch keine Bewertungen
- Syarah Hikam 1Dokument108 SeitenSyarah Hikam 1AuliaRahmanNoch keine Bewertungen
- Igra Factsheet Oct2011 PDFDokument2 SeitenIgra Factsheet Oct2011 PDFAuliaRahmanNoch keine Bewertungen
- Interesting Case March, 15 2016: Sri Yati, Charles, Aulia, Fanny, SasaDokument31 SeitenInteresting Case March, 15 2016: Sri Yati, Charles, Aulia, Fanny, SasaAuliaRahmanNoch keine Bewertungen
- Interesting Case March, 15 2016: Sri Yati, Charles, Aulia, Fanny, SasaDokument31 SeitenInteresting Case March, 15 2016: Sri Yati, Charles, Aulia, Fanny, SasaAuliaRahmanNoch keine Bewertungen
- NEWSDokument183 SeitenNEWSSebastian BaqueroNoch keine Bewertungen
- bRAIN gYMDokument11 SeitenbRAIN gYMshannay201050% (2)
- Breastfeeding: Best For Baby and MotherDokument12 SeitenBreastfeeding: Best For Baby and MotherSari Whardani Mahligai PateryNoch keine Bewertungen
- Diagnosis of Childhood Acute Lymphoblastic Leukemia and Optimization of Risk-Benefit Ratio of TherapyDokument24 SeitenDiagnosis of Childhood Acute Lymphoblastic Leukemia and Optimization of Risk-Benefit Ratio of TherapyAuliaRahmanNoch keine Bewertungen
- Igra Factsheet Oct2011Dokument2 SeitenIgra Factsheet Oct2011AuliaRahmanNoch keine Bewertungen
- Incase Qobam Lab 17 MaretDokument6 SeitenIncase Qobam Lab 17 MaretAuliaRahmanNoch keine Bewertungen
- Varicella Vaccination AlgorithmDokument1 SeiteVaricella Vaccination AlgorithmAuliaRahmanNoch keine Bewertungen
- Wilayah 3'-DiterjemahkanDokument1 SeiteWilayah 3'-DiterjemahkanAuliaRahmanNoch keine Bewertungen
- Interesting Case: Masruri, Esha, Alex, Milza, Wicak, Gita, Zaki, Arin, Eni, FiaDokument10 SeitenInteresting Case: Masruri, Esha, Alex, Milza, Wicak, Gita, Zaki, Arin, Eni, FiaAuliaRahmanNoch keine Bewertungen
- Interesting Case 27.03.2013Dokument10 SeitenInteresting Case 27.03.2013AuliaRahmanNoch keine Bewertungen
- Pediatric Dental CareDokument27 SeitenPediatric Dental CareAuliaRahmanNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
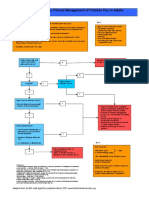
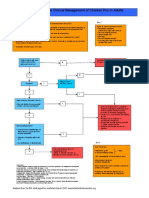
- Pediatric Type 1 Diabetes MellitusDokument25 SeitenPediatric Type 1 Diabetes MellitusmuhammadferhatNoch keine Bewertungen
- CC CCCCC: Y CCC CCCC CCCCC CCCC CCC CCCCCCCCCC CC CDokument3 SeitenCC CCCCC: Y CCC CCCC CCCCC CCCC CCC CCCCCCCCCC CC CRachel Ann BatayolaNoch keine Bewertungen
- QR Management of Type 2 Diabetes Mellitus (5th Edition) PDFDokument8 SeitenQR Management of Type 2 Diabetes Mellitus (5th Edition) PDFKai Xin100% (1)
- 2018 Clinical Practice Guidelines: Diabetes in Older PeopleDokument35 Seiten2018 Clinical Practice Guidelines: Diabetes in Older Peopledodi ikhsanNoch keine Bewertungen
- Long Term DiabetesDokument68 SeitenLong Term Diabetesnawaraj2044Noch keine Bewertungen
- Acute Complication of Diabetes MellitusDokument37 SeitenAcute Complication of Diabetes MellitusImron RosyadiNoch keine Bewertungen
- Type Ii Diabetes MellitusDokument2 SeitenType Ii Diabetes MellitusBeverly CalmaNoch keine Bewertungen
- Diabetes Mellitus DescritionDokument5 SeitenDiabetes Mellitus DescritionTinke WinkeNoch keine Bewertungen
- The Role of Insulin in Maintaining Blood Glucose HomeostasisDokument2 SeitenThe Role of Insulin in Maintaining Blood Glucose HomeostasisyaniqueNoch keine Bewertungen
- Study Guide Blood Glucose MonitoringDokument4 SeitenStudy Guide Blood Glucose MonitoringDan Dan ManaoisNoch keine Bewertungen
- ISPAD Clinical Practice Consensus Guidelines 2018: Management of Children and Adolescents With Diabetes Requiring SurgeryDokument10 SeitenISPAD Clinical Practice Consensus Guidelines 2018: Management of Children and Adolescents With Diabetes Requiring SurgeryAbdi KebedeNoch keine Bewertungen
- 1-Definition Epidemiology and Classification of Diabetes in Children and Adolescents PDFDokument14 Seiten1-Definition Epidemiology and Classification of Diabetes in Children and Adolescents PDFFrancys Sierra FariasNoch keine Bewertungen
- Diabetes in Pregnancy: DR Omar Abu-AzzamDokument36 SeitenDiabetes in Pregnancy: DR Omar Abu-AzzamRoba Mohmed AlamroNoch keine Bewertungen
- Gambaran Status Gizi Pasien Diabetes Melitus Tipe 2 Berdasarkan AntropometriDokument7 SeitenGambaran Status Gizi Pasien Diabetes Melitus Tipe 2 Berdasarkan AntropometriIntan PratiwiNoch keine Bewertungen
- Find Diabitis Revrsal Prog3Dokument2 SeitenFind Diabitis Revrsal Prog3Jani AmitkumarNoch keine Bewertungen
- Prediabetes A High Risk State For Diabetes Development PDFDokument12 SeitenPrediabetes A High Risk State For Diabetes Development PDFDario Neri CortezNoch keine Bewertungen
- 397 251079 1 10 20211231Dokument7 Seiten397 251079 1 10 20211231ariaNoch keine Bewertungen
- Diabetes Mellit-Wps OfficeDokument8 SeitenDiabetes Mellit-Wps OfficeSulthana Rasiya NNoch keine Bewertungen
- Gestational Diabetes Mellitus PathophysiologyDokument1 SeiteGestational Diabetes Mellitus PathophysiologyAntonette CedroNoch keine Bewertungen
- Diabetes PPT FianlDokument31 SeitenDiabetes PPT FianlUqba MishalNoch keine Bewertungen
- IDF Atlas 10th Edition Presentation V11Dokument23 SeitenIDF Atlas 10th Edition Presentation V11revathy deivasigamaniNoch keine Bewertungen
- NCM 118 - Lesson 13 (DKA and HHNS)Dokument3 SeitenNCM 118 - Lesson 13 (DKA and HHNS)Bobby Christian DuronNoch keine Bewertungen
- Insulin in GDM Ver 2.0Dokument47 SeitenInsulin in GDM Ver 2.0Akash GuptaNoch keine Bewertungen
- Informationfordoctors Revised April14Dokument2 SeitenInformationfordoctors Revised April14Mesfin DerbewNoch keine Bewertungen
- HypoglycaemiaDokument3 SeitenHypoglycaemiaAneejaa BidhaNoch keine Bewertungen
- Hyperosmolar Hyperglycemic StateDokument13 SeitenHyperosmolar Hyperglycemic Stateanon_903760906Noch keine Bewertungen
- 58-Article Text-169-1-10-20180804Dokument8 Seiten58-Article Text-169-1-10-20180804grace nazaviraNoch keine Bewertungen
- Study of Coagulation Profile in Type 2 Diabetes Mellitus Patients in Correlation With Long Term Glycemic Control (Hba1c)Dokument2 SeitenStudy of Coagulation Profile in Type 2 Diabetes Mellitus Patients in Correlation With Long Term Glycemic Control (Hba1c)IJAR JOURNALNoch keine Bewertungen
- Cookies Tepung Beras Hitam Dan Kedelai HDokument10 SeitenCookies Tepung Beras Hitam Dan Kedelai HBrian Mukti NugrohoNoch keine Bewertungen
- Yale IIP MICU120-160 2011Dokument2 SeitenYale IIP MICU120-160 2011afm26Noch keine Bewertungen