Das könnte Ihnen auch gefallen
- The Children's Hospital of Philadelphia Guide to Asthma: How to Help Your Child Live a Healthier LifeVon EverandThe Children's Hospital of Philadelphia Guide to Asthma: How to Help Your Child Live a Healthier LifeJulian Lewis Allen, M.D.Noch keine Bewertungen
- Apnea 2019Dokument10 SeitenApnea 2019aiswarya sreekumarNoch keine Bewertungen
- Postpartum DisordersDokument68 SeitenPostpartum DisordersPrecious SorianoNoch keine Bewertungen
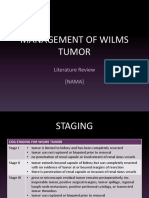
- Management of Wilms Tumor: Literature Review (NAMA)Dokument15 SeitenManagement of Wilms Tumor: Literature Review (NAMA)DeaNataliaNoch keine Bewertungen
- High Risk Newborn - Study GuideDokument10 SeitenHigh Risk Newborn - Study GuideMalou Yap Buot100% (1)
- Beta Thalassemia: DefinitionDokument9 SeitenBeta Thalassemia: Definitioncelestina dawn peterNoch keine Bewertungen
- What Is Covid-19Dokument5 SeitenWhat Is Covid-19Aunia Putri HemasNoch keine Bewertungen
- Coronavirus Disease 2019 (COVID-19) : Because Learning Changes EverythingDokument29 SeitenCoronavirus Disease 2019 (COVID-19) : Because Learning Changes EverythingDennis MuthusiNoch keine Bewertungen
- Care of Clients With Alterations in Oxygen Carrying Capacity (Hematologic Disorder)Dokument30 SeitenCare of Clients With Alterations in Oxygen Carrying Capacity (Hematologic Disorder)Michael John CanlasNoch keine Bewertungen
- Genetics: (Percentage Breakdown of Overall Hemophilia Population by Severity)Dokument2 SeitenGenetics: (Percentage Breakdown of Overall Hemophilia Population by Severity)uikgykNoch keine Bewertungen
- Subinvolution of The UterusDokument5 SeitenSubinvolution of The UterusJanica Rose Maloloy-onNoch keine Bewertungen
- Acute Management of Burns in ChildrenDokument52 SeitenAcute Management of Burns in ChildrenJonie Vince SañosaNoch keine Bewertungen
- ThalassemiaDokument16 SeitenThalassemiaAry AffandiNoch keine Bewertungen
- Infants Diabetic MothersDokument17 SeitenInfants Diabetic MothersJaya PrabhaNoch keine Bewertungen
- Rheumatic FeverDokument15 SeitenRheumatic FeverJeaneta Cheryl PatrickNoch keine Bewertungen
- High Risk Newborn: Dr. H. Usha RaniDokument28 SeitenHigh Risk Newborn: Dr. H. Usha RaniNaresh GadaganiNoch keine Bewertungen
- Thalassemia 20-05-2020Dokument164 SeitenThalassemia 20-05-2020Mohd Anas SheikhNoch keine Bewertungen
- Hemophilia ADokument29 SeitenHemophilia ASari RakhmawatiNoch keine Bewertungen
- MCNDokument12 SeitenMCNIan CarodanNoch keine Bewertungen
- ThalassemiaDokument24 SeitenThalassemiaapi-459076195Noch keine Bewertungen
- Pneumonia in ChildrenDokument4 SeitenPneumonia in ChildrenkuterinbatNoch keine Bewertungen
- Rheumatic Heart DiseaseDokument2 SeitenRheumatic Heart DiseaseDiaz RahmadiNoch keine Bewertungen
- Breastfeeding and HivDokument30 SeitenBreastfeeding and HivbxrbxrNoch keine Bewertungen
- High Risk Newborn Conditions Present at BirthDokument47 SeitenHigh Risk Newborn Conditions Present at BirthChinchu ChinchuNoch keine Bewertungen
- Pediatric Respiratory Disorders General InterventionsDokument2 SeitenPediatric Respiratory Disorders General Interventionscayla mae carlosNoch keine Bewertungen
- Case Study 2Dokument3 SeitenCase Study 2jamesNoch keine Bewertungen
- 7-Neonatal Surgical EmergenciesDokument29 Seiten7-Neonatal Surgical EmergenciesResti Rangga SusiloNoch keine Bewertungen
- 3M CVP Monitoring - Assisting in BMA ECG Interpretation - Final Draft - 3CDokument65 Seiten3M CVP Monitoring - Assisting in BMA ECG Interpretation - Final Draft - 3CAlexa GoteraNoch keine Bewertungen
- MedSurg Chapter 51 OutlineDokument7 SeitenMedSurg Chapter 51 OutlineJosephine Navarro100% (1)
- Labor and Delivery 34: Removing OvariesDokument3 SeitenLabor and Delivery 34: Removing OvariesDianneNoch keine Bewertungen
- Wilms Tumour: Nitha K 2 Year MSC NursingDokument40 SeitenWilms Tumour: Nitha K 2 Year MSC NursingNITHA K100% (1)
- Clinician'S Guide: Asthma Management GuidelinesDokument16 SeitenClinician'S Guide: Asthma Management GuidelinesNata1511Noch keine Bewertungen
- NCP CaseDokument34 SeitenNCP CaseIsobel Mae JacelaNoch keine Bewertungen
- Monitoring The Progress of Labor: Marissa Villacarlos Nualla, MD, Fpogs, Fpsuog Mcu-College of MedicineDokument58 SeitenMonitoring The Progress of Labor: Marissa Villacarlos Nualla, MD, Fpogs, Fpsuog Mcu-College of MedicineRozzie ReyesNoch keine Bewertungen
- Meconium AspirationDokument23 SeitenMeconium AspirationWitneyGraceNoch keine Bewertungen
- Or Technique Scrubbing, Gowning and Arranging Instruments: 1. Define The Following Terms: Peri - Operative NursingDokument35 SeitenOr Technique Scrubbing, Gowning and Arranging Instruments: 1. Define The Following Terms: Peri - Operative NursingHoney MacabuhayNoch keine Bewertungen
- Puerperal InfectionDokument28 SeitenPuerperal InfectionputriNoch keine Bewertungen
- NURS 3337 Day1 WorkbookDokument18 SeitenNURS 3337 Day1 WorkbookEmerald Holly TagoNoch keine Bewertungen
- JaundiceDokument41 SeitenJaundicesavina hasbianiNoch keine Bewertungen
- Child With Respiratory DysfunctionDokument23 SeitenChild With Respiratory DysfunctionmeganNoch keine Bewertungen
- 2.2 NCM 109 - Complications During Pregnancy, Labor and Delivery and Postpartum PeriodsDokument10 Seiten2.2 NCM 109 - Complications During Pregnancy, Labor and Delivery and Postpartum PeriodsSittie Haneen TabaraNoch keine Bewertungen
- Newborn AssessmentDokument5 SeitenNewborn Assessmentlanilyn aquinoNoch keine Bewertungen
- Maternity - Postnatal Care in The First Week - CG - 2015Dokument41 SeitenMaternity - Postnatal Care in The First Week - CG - 2015Monica SurduNoch keine Bewertungen
- Drugs in The Neonatal Unit: 1 Julia PettyDokument5 SeitenDrugs in The Neonatal Unit: 1 Julia PettyMarjoNoch keine Bewertungen
- A Middle-Range Theory of Self-Care ofDokument24 SeitenA Middle-Range Theory of Self-Care ofARIKANoch keine Bewertungen
- Infant of Diabetic MotherDokument14 SeitenInfant of Diabetic MothersreekalaNoch keine Bewertungen
- Transient Tachypnea of NewbornsDokument16 SeitenTransient Tachypnea of NewbornsSelena Marie0% (1)
- 8. Care of Child With GI Dysfunction (1) ءءءءDokument44 Seiten8. Care of Child With GI Dysfunction (1) ءءءءNuhaNoch keine Bewertungen
- Management of Neonatal HypoglycemiaDokument14 SeitenManagement of Neonatal Hypoglycemiaece142Noch keine Bewertungen
- DOH Maternal Health ProgramDokument5 SeitenDOH Maternal Health ProgramErwin Jake TagubaNoch keine Bewertungen
- Fetal Monitoring Orientation Day-1Dokument50 SeitenFetal Monitoring Orientation Day-1Scott CalfeeNoch keine Bewertungen
- RESPIRATORY DISORDERS (Abdurahman S)Dokument19 SeitenRESPIRATORY DISORDERS (Abdurahman S)Rahmat MuliaNoch keine Bewertungen
- Pre and Post PregnancyDokument23 SeitenPre and Post PregnancyJitendra ChaudharyNoch keine Bewertungen
- Intrapartal PeriodDokument2 SeitenIntrapartal PeriodLeah ElizabethNoch keine Bewertungen
- Care of Clients With Problem in Oxygenation Quiz 3Dokument5 SeitenCare of Clients With Problem in Oxygenation Quiz 3marsan12Noch keine Bewertungen
- Wilms TumorDokument38 SeitenWilms TumorEjay Jacob RicamaraNoch keine Bewertungen
- Maternal and Child Heath: Jay Pee C. Malibiran Nurse 1 RNDokument36 SeitenMaternal and Child Heath: Jay Pee C. Malibiran Nurse 1 RNRosebel Lagura100% (1)
- Eming Report Precipitous LaborDokument11 SeitenEming Report Precipitous LaborJudeLaxNoch keine Bewertungen
- Complications in PregnancyDokument81 SeitenComplications in PregnancyTia TahniaNoch keine Bewertungen
- Perspective Plan 2022-27Dokument57 SeitenPerspective Plan 2022-27So kharap kuchNoch keine Bewertungen
- Careers in Biomedical ScienceDokument24 SeitenCareers in Biomedical ScienceEncik LaLaNoch keine Bewertungen
- High Blood Pressure Screening PackageDokument1 SeiteHigh Blood Pressure Screening PackageAlita PalpialyNoch keine Bewertungen
- BCSE Study Strategies Zuku ReviewDokument61 SeitenBCSE Study Strategies Zuku ReviewNayara Pataro91% (11)
- Drug Regulatory Agency of Pakistan (DRAP)Dokument12 SeitenDrug Regulatory Agency of Pakistan (DRAP)Mrs YezdaniNoch keine Bewertungen
- National Institute of Ayurveda: BrochureDokument10 SeitenNational Institute of Ayurveda: BrochureKopal AgarwalNoch keine Bewertungen
- Johnmar Abuan Health Activity 1: Ready To Go Situation 1Dokument10 SeitenJohnmar Abuan Health Activity 1: Ready To Go Situation 1Katherine B. AbuanNoch keine Bewertungen
- Garuda 762976Dokument5 SeitenGaruda 762976bimaNoch keine Bewertungen
- Fee Paying FreshDokument3 SeitenFee Paying FreshQuame HazyNoch keine Bewertungen
- Sincope Vs Crisis - Lancet Neurol 2006 PDFDokument10 SeitenSincope Vs Crisis - Lancet Neurol 2006 PDFLina HerreraNoch keine Bewertungen
- Supply Exam Time Table 2021Dokument2 SeitenSupply Exam Time Table 2021Sudda8 KumaraNoch keine Bewertungen
- PneumoniaDokument27 SeitenPneumoniamameekasim75Noch keine Bewertungen
- Nursing Diagnosis # 1 Acute Pain Related To Abdominal Incision.Dokument10 SeitenNursing Diagnosis # 1 Acute Pain Related To Abdominal Incision.jhunanax100% (3)
- Explanation 2020 1Dokument315 SeitenExplanation 2020 1Reshma Shaji PnsNoch keine Bewertungen
- Factfile 1: Mental Health and EmploymentDokument4 SeitenFactfile 1: Mental Health and Employmenttony_jameson-allenNoch keine Bewertungen
- National Leprosy Eradication Program (Nlep: Dr. Kanupriya ChaturvediDokument24 SeitenNational Leprosy Eradication Program (Nlep: Dr. Kanupriya ChaturvediLavendra KunwarNoch keine Bewertungen
- Leva FlukeDokument5 SeitenLeva FlukeراجيرحمةربهNoch keine Bewertungen
- Clin Infect Dis. 2007 Gupta 241 9Dokument9 SeitenClin Infect Dis. 2007 Gupta 241 9Handy SaputraNoch keine Bewertungen
- The Information System and Surveillance System in Community Health CareDokument14 SeitenThe Information System and Surveillance System in Community Health CareNamayanja SumayiyahNoch keine Bewertungen
- Bupropion Hydrochloride (Drug Study)Dokument3 SeitenBupropion Hydrochloride (Drug Study)Franz.thenurse6888100% (1)
- Ujian Snake Bite RusmitaDokument33 SeitenUjian Snake Bite RusmitaArina TsusayyaNoch keine Bewertungen
- Exam Semi23423123132Dokument2 SeitenExam Semi23423123132gwapoNoch keine Bewertungen
- BPSA-CGT 2018 Poster Cell & Gene Therapy Process Map PDFDokument1 SeiteBPSA-CGT 2018 Poster Cell & Gene Therapy Process Map PDFbioNoch keine Bewertungen
- A Sensible and Compassionate Anti-COVID Strategy: My GoalDokument6 SeitenA Sensible and Compassionate Anti-COVID Strategy: My GoalZarrar KhanNoch keine Bewertungen
- Revistas Isi PDFDokument298 SeitenRevistas Isi PDFMichele WrightNoch keine Bewertungen
- Nutrition Assessment Lab 2Dokument10 SeitenNutrition Assessment Lab 2Lee Yann LynnNoch keine Bewertungen
- Polycystic Ovary SyndromeDokument11 SeitenPolycystic Ovary SyndromeABC11Noch keine Bewertungen
- Lecture1 2 Advancedemergencytraumacourse Introductionandcourseoverview 1Dokument66 SeitenLecture1 2 Advancedemergencytraumacourse Introductionandcourseoverview 1vikoraNoch keine Bewertungen
- Medico Legal Aspects of Severe Traumatic Brain InjuryDokument17 SeitenMedico Legal Aspects of Severe Traumatic Brain InjuryIrv CantorNoch keine Bewertungen
- Faring It IsDokument8 SeitenFaring It IsMuhammad sukronNoch keine Bewertungen