Das könnte Ihnen auch gefallen
- UEE62111 4 SummaryDokument4 SeitenUEE62111 4 SummarySasho GjorgjievskiNoch keine Bewertungen
- O I ElgerdDokument109 SeitenO I ElgerdShyam KumarNoch keine Bewertungen
- A2 - PovertyDokument1 SeiteA2 - PovertySasho GjorgjievskiNoch keine Bewertungen
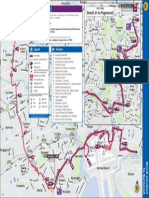
- Bondi JN To Pagewood: Legend SectionsDokument1 SeiteBondi JN To Pagewood: Legend SectionsSasho GjorgjievskiNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Henna, Lawsonia Inermis1Dokument28 SeitenHenna, Lawsonia Inermis1zaheeda1984Noch keine Bewertungen
- Gastrointestinal Infections & Viral Hepatitis: Prof. Dr. Sabiha Pit Medical Microbiology Session 2008/2009Dokument25 SeitenGastrointestinal Infections & Viral Hepatitis: Prof. Dr. Sabiha Pit Medical Microbiology Session 2008/2009Khadyjah RashidNoch keine Bewertungen
- Invisible Minerals Part I Magnesium: DisclaimerDokument119 SeitenInvisible Minerals Part I Magnesium: DisclaimerhemanthalNoch keine Bewertungen
- Are There Medicines To Treat Infection With Flu?: 800-CDC-INFODokument2 SeitenAre There Medicines To Treat Infection With Flu?: 800-CDC-INFOMaria Chacón CarbajalNoch keine Bewertungen
- Women S Health MidtermDokument30 SeitenWomen S Health MidtermKatarzyna CiesielskaNoch keine Bewertungen
- Presentation On: Pueperal Sepsis: Submitted To: Sandhya Maam Submitted By: Dhana BC Kismita Rai BSC 3 YearDokument31 SeitenPresentation On: Pueperal Sepsis: Submitted To: Sandhya Maam Submitted By: Dhana BC Kismita Rai BSC 3 YearRumi Maharjan100% (1)
- Bacteriology SummaryDokument38 SeitenBacteriology SummaryMohsen HaleemNoch keine Bewertungen
- Thyroid Function Tests (TFTS)Dokument27 SeitenThyroid Function Tests (TFTS)ธิติวุฒิ แสงคล้อยNoch keine Bewertungen
- Medicine Simplified DBMCI: To Get More Content Like This Join Our Telegram GroupDokument8 SeitenMedicine Simplified DBMCI: To Get More Content Like This Join Our Telegram GroupAnisa Osman HassanNoch keine Bewertungen
- Epidemiology For MPH StudentsDokument91 SeitenEpidemiology For MPH StudentsteklayNoch keine Bewertungen
- Slaber Jaga Senin 3 Mei 2021Dokument7 SeitenSlaber Jaga Senin 3 Mei 2021Louis MailuhuNoch keine Bewertungen
- Best of Five MCQs For The Geriatric Medicine SCE-Oxford University Press (2014)Dokument284 SeitenBest of Five MCQs For The Geriatric Medicine SCE-Oxford University Press (2014)Raihan Isvandiar100% (2)
- PDF DIR 456Dokument6 SeitenPDF DIR 456Fauzan MaulanaNoch keine Bewertungen
- Primary Psoas Abscess: Alexandru Crisan, Emilia Nicoara, Karina Bota, Doru BordosDokument3 SeitenPrimary Psoas Abscess: Alexandru Crisan, Emilia Nicoara, Karina Bota, Doru BordosNataliaMaedyNoch keine Bewertungen
- EDUC 104 Report (Nik&Jeh)Dokument48 SeitenEDUC 104 Report (Nik&Jeh)Nikki DanaNoch keine Bewertungen
- BotoxDokument18 SeitenBotoxNikita AggarwalNoch keine Bewertungen
- Classification Criteria For Sjogrens Syndrome A RDokument7 SeitenClassification Criteria For Sjogrens Syndrome A RYafanita IzzatiNoch keine Bewertungen
- Medical Terms in Lay Language2Dokument7 SeitenMedical Terms in Lay Language2Mavra zNoch keine Bewertungen
- Cardio Notes 2Dokument11 SeitenCardio Notes 2AngieNoch keine Bewertungen
- Visceral Pain Somatic Pain Referred Pain: 9. Acute AbdomenDokument4 SeitenVisceral Pain Somatic Pain Referred Pain: 9. Acute AbdomenLenard BangugNoch keine Bewertungen
- Health Care Disparities PaperDokument8 SeitenHealth Care Disparities Paperapi-235633705Noch keine Bewertungen
- Nature's Pathways Mar 2012 Issue - Northeast WI EditionDokument100 SeitenNature's Pathways Mar 2012 Issue - Northeast WI EditionNature's PathwaysNoch keine Bewertungen
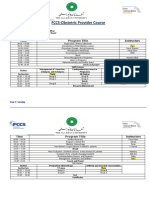
- FCCS-Obstetric Provider Course: Time Program Title InstructorsDokument2 SeitenFCCS-Obstetric Provider Course: Time Program Title InstructorsSamina AyazNoch keine Bewertungen
- Slide Kuliah FK USU ArrhythmiaDokument40 SeitenSlide Kuliah FK USU ArrhythmiaYolanda SimamoraNoch keine Bewertungen
- 4th Grading Grade 8Dokument1 Seite4th Grading Grade 8Gissele AbolucionNoch keine Bewertungen
- Paracetamol PoisoningDokument12 SeitenParacetamol PoisoningOoi Ah GuanNoch keine Bewertungen
- Digestive System DiseasesDokument2 SeitenDigestive System DiseasesPRINTDESK by DanNoch keine Bewertungen
- Combating COVID-19 and Building Immune Resilience: A Potential Role For Magnesium Nutrition?Dokument10 SeitenCombating COVID-19 and Building Immune Resilience: A Potential Role For Magnesium Nutrition?witaNoch keine Bewertungen
- EndocrineDokument55 SeitenEndocrineKolapo SanusiNoch keine Bewertungen
- Genital Herpes: Alyster Balingit Rosemarie de GuzmanDokument11 SeitenGenital Herpes: Alyster Balingit Rosemarie de GuzmanAlyster BalingitNoch keine Bewertungen