Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Daftar PustakaDokument2 SeitenDaftar PustakaMeylinda LinNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Artritis Enteropati: Karen Atkinson, MD, MPHDokument22 SeitenArtritis Enteropati: Karen Atkinson, MD, MPHMeylinda LinNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- DapusDokument1 SeiteDapusMeylinda LinNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Artritis Enteropati: Karen Atkinson, MD, MPHDokument22 SeitenArtritis Enteropati: Karen Atkinson, MD, MPHMeylinda LinNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Panduan Tutorial CDokument6 SeitenPanduan Tutorial CMeylinda LinNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Malignant HyperthermiaDokument20 SeitenMalignant HyperthermiaMeylinda Lin100% (1)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- IDcardDokument1 SeiteIDcardMeylinda LinNoch keine Bewertungen
- Evaluation Liver Function TestsDokument74 SeitenEvaluation Liver Function TestsMeylinda LinNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Patofisiologi Malaria PDFDokument11 SeitenPatofisiologi Malaria PDFMeylinda LinNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- General Principles of Motivation: by Matthew Weller, Los Angeles Business Journal, March 14, 2005Dokument6 SeitenGeneral Principles of Motivation: by Matthew Weller, Los Angeles Business Journal, March 14, 2005Meylinda LinNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- A Plan of Life - Scepter BookletDokument10 SeitenA Plan of Life - Scepter Bookletpeteatkinson@gmail.comNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Exploration of MoonDokument8 SeitenExploration of MoonAryan KhannaNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
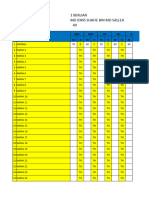
- TEMPLATE Keputusan Peperiksaan THP 1Dokument49 SeitenTEMPLATE Keputusan Peperiksaan THP 1SABERI BIN BANDU KPM-GuruNoch keine Bewertungen
- OsteomyelitisDokument10 SeitenOsteomyelitismustafaNoch keine Bewertungen
- 39 Storey Treehouse Activity Pack PDFDokument11 Seiten39 Storey Treehouse Activity Pack PDFNeptune Shell0% (3)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Blood TestsDokument3 SeitenBlood TestsMarycharinelle Antolin MolinaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Filed: Patrick FisherDokument12 SeitenFiled: Patrick FisherScribd Government DocsNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Indian RailwaysDokument20 SeitenIndian RailwaysNirmalNoch keine Bewertungen
- (NewResultBD - Com) Mymensingh Board JSC Scholarship Result 2019Dokument80 Seiten(NewResultBD - Com) Mymensingh Board JSC Scholarship Result 2019rthedthbdeth100% (1)
- Making A Spiritual ConfessionDokument2 SeitenMaking A Spiritual ConfessionJoselito FernandezNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- PETITION For Declaration of NullityDokument7 SeitenPETITION For Declaration of NullityKira Jorgio100% (3)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- Introduction To Strategic Cost Management and Management AccountingDokument3 SeitenIntroduction To Strategic Cost Management and Management AccountingnovyNoch keine Bewertungen
- Whether To Use Their GPS To Find Their Way To The New Cool Teen HangoutDokument3 SeitenWhether To Use Their GPS To Find Their Way To The New Cool Teen HangoutCarpovici Victor100% (1)
- 7999 Cswdo Day CareDokument3 Seiten7999 Cswdo Day CareCharles D. FloresNoch keine Bewertungen
- Sec A - Group 9 - When A New Manager StumblesDokument13 SeitenSec A - Group 9 - When A New Manager StumblesVijay Krishnan100% (3)
- MEM Companion Volume Implementation Guide - Release 1.1Dokument23 SeitenMEM Companion Volume Implementation Guide - Release 1.1Stanley AlexNoch keine Bewertungen
- Financial Fitness ChecklistDokument4 SeitenFinancial Fitness Checklistcoach_22Noch keine Bewertungen
- UnderstandQUIC MoreDokument12 SeitenUnderstandQUIC MoreONEmillion knowledgeNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- English Full Book PaperDokument2 SeitenEnglish Full Book PaperSaira BatoolNoch keine Bewertungen
- D245S 734046 Om enDokument90 SeitenD245S 734046 Om enEndro Accoustic100% (1)
- New Microsoft Office Word DocumentDokument3 SeitenNew Microsoft Office Word DocumentVince Vince100% (1)
- Knock Knock GamesDokument1 SeiteKnock Knock GamesArsyta AnandaNoch keine Bewertungen
- Question Paper Code:: (10×2 20 Marks)Dokument2 SeitenQuestion Paper Code:: (10×2 20 Marks)Umesh Harihara sudan0% (1)
- Flore Bridoux CV Sep 2016 Short VersionDokument10 SeitenFlore Bridoux CV Sep 2016 Short Versionbayu_pancaNoch keine Bewertungen
- Juzaili Alias SSB Jadual Perubahan PDP Dan Penilaian AlternatifDokument1 SeiteJuzaili Alias SSB Jadual Perubahan PDP Dan Penilaian Alternatifkar afiNoch keine Bewertungen
- Answer Sheet RRLDokument2 SeitenAnswer Sheet RRLDolores PanchoNoch keine Bewertungen
- Indian Board of Alternative Medicine: Partner-Pub-1166 ISO-8859-1Dokument14 SeitenIndian Board of Alternative Medicine: Partner-Pub-1166 ISO-8859-1vipinNoch keine Bewertungen
- Everyday Use AnalysisDokument8 SeitenEveryday Use AnalysisThe 3d PlanetNoch keine Bewertungen
- The Honey Gatherers - Travels With The Bauls - The Wandering Minstrels of Rural India - Mimlu Sen PDFDokument16 SeitenThe Honey Gatherers - Travels With The Bauls - The Wandering Minstrels of Rural India - Mimlu Sen PDFAurko F AhmadNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Camp High Harbour at Lake LanierDokument3 SeitenCamp High Harbour at Lake LaniermetroatlantaymcaNoch keine Bewertungen