Das könnte Ihnen auch gefallen
- Motor Neuron DiseaseDokument22 SeitenMotor Neuron DiseaseNabin SimkhadaNoch keine Bewertungen
- KortikospinalisDokument4 SeitenKortikospinalisAhmad SaifulNoch keine Bewertungen
- Kepaniteraan Klinik RSD Mardi Waluyo Blitar - FK Unisma: Pembimbing: Dr. Utchu Tedja Mulya SP.BDokument35 SeitenKepaniteraan Klinik RSD Mardi Waluyo Blitar - FK Unisma: Pembimbing: Dr. Utchu Tedja Mulya SP.BDada DoniNoch keine Bewertungen
- MNJ ToastDokument4 SeitenMNJ ToastRichard SuherlimNoch keine Bewertungen
- Neuroanatomi AriesDokument48 SeitenNeuroanatomi AriesAries Rahman HakimNoch keine Bewertungen
- Sturge Weber SyndromeDokument14 SeitenSturge Weber SyndromeAnumeha JindalNoch keine Bewertungen
- Hubungan Antara Kualitas Tidur Dengan Keparahan StrokeDokument8 SeitenHubungan Antara Kualitas Tidur Dengan Keparahan StrokeadindaanjaniNoch keine Bewertungen
- MYELITISDokument8 SeitenMYELITISFebrina RamadhaniNoch keine Bewertungen
- Neuroradiology: Sony Sutrisno Department of Radiology Krida Wacana Christian UniversityDokument46 SeitenNeuroradiology: Sony Sutrisno Department of Radiology Krida Wacana Christian UniversityPaulus AnungNoch keine Bewertungen
- Trauma Medula SpinalisDokument33 SeitenTrauma Medula Spinalisintan rizka ndNoch keine Bewertungen
- Kuesioner NandaDokument8 SeitenKuesioner NandaAnanda AsmaraNoch keine Bewertungen
- Dasar-Dasar Membaca Elektroensefalografi - Gea Pandhita SDokument84 SeitenDasar-Dasar Membaca Elektroensefalografi - Gea Pandhita Sgea pandhita sNoch keine Bewertungen
- k20 - Stroke IskemikDokument35 Seitenk20 - Stroke IskemikZikri Putra Lan LubisNoch keine Bewertungen
- Kriteria Diagnostik McDonald 2017Dokument8 SeitenKriteria Diagnostik McDonald 2017SMF BEDAH SoebandiNoch keine Bewertungen
- Neurotoksikologi: DR - Sandi Lesmana, SP.SDokument48 SeitenNeurotoksikologi: DR - Sandi Lesmana, SP.Sdita anisya putriNoch keine Bewertungen
- Neuroanatomi 2011Dokument51 SeitenNeuroanatomi 2011Farah MuthiaNoch keine Bewertungen
- MiopatiDokument7 SeitenMiopatiMarco HutagaolNoch keine Bewertungen
- Scoring BPSDDokument4 SeitenScoring BPSDayu yuliantiNoch keine Bewertungen
- Laporan Kasus - Buta KortikalDokument31 SeitenLaporan Kasus - Buta KortikalwadejackNoch keine Bewertungen
- CK 7 and CK 20 Positive Tumors Modern Pathol 2000Dokument11 SeitenCK 7 and CK 20 Positive Tumors Modern Pathol 2000api-26176346Noch keine Bewertungen
- Anatomy of The Mental and Neurobehavior DisordersDokument57 SeitenAnatomy of The Mental and Neurobehavior DisordersiqiqiqiqiqNoch keine Bewertungen
- BLOK 1.3 Jaras PenglihatanDokument43 SeitenBLOK 1.3 Jaras PenglihatanlenypsNoch keine Bewertungen
- 3rd Announcement Konas-IX PerdossiDokument30 Seiten3rd Announcement Konas-IX PerdossiA Hadid FirdiyanshahNoch keine Bewertungen
- Dr. Heny - Referred PainDokument15 SeitenDr. Heny - Referred PainAnonymous FfZm5kOkYFNoch keine Bewertungen
- Pre KKD I - Baru NeuroDokument81 SeitenPre KKD I - Baru NeuroancillaagraynNoch keine Bewertungen
- Neuro Part 1Dokument5 SeitenNeuro Part 1rigilkent28Noch keine Bewertungen
- Ohtahara Syndrome: Corticosteroids (Prednisolone or ACTH) Are Occasionally HelpfulDokument2 SeitenOhtahara Syndrome: Corticosteroids (Prednisolone or ACTH) Are Occasionally HelpfulidscribddotcomNoch keine Bewertungen
- KKD NeuroDokument22 SeitenKKD NeuroFerdyNoch keine Bewertungen
- Responsi NeuroanatomiDokument36 SeitenResponsi Neuroanatomiajik_ndut89Noch keine Bewertungen
- Critical Appraisal PrognosisDokument15 SeitenCritical Appraisal PrognosismortazaqNoch keine Bewertungen
- Interpretasi Foto TulangDokument35 SeitenInterpretasi Foto TulanganwarNoch keine Bewertungen
- Imaging of Normal SpineDokument32 SeitenImaging of Normal SpineDestia AnandaNoch keine Bewertungen
- Embriologi Umum: Dr. Thontowi Djauhari NS, MkesDokument63 SeitenEmbriologi Umum: Dr. Thontowi Djauhari NS, Mkesteteh_pratamiNoch keine Bewertungen
- Pyramidal TractDokument48 SeitenPyramidal TractdenekeNoch keine Bewertungen
- Tatalaksana Cairan Dan ElektrolitDokument42 SeitenTatalaksana Cairan Dan ElektrolitHerizko Kusuma0% (1)
- Referat Tumor Sinus CavernousDokument6 SeitenReferat Tumor Sinus CavernousImam Adi NugrohoNoch keine Bewertungen
- Dr. Kiki Mohammad Iqbal, SPS: Departemen Neurologi FK Usu / Rsup H. Adam Malik MedanDokument35 SeitenDr. Kiki Mohammad Iqbal, SPS: Departemen Neurologi FK Usu / Rsup H. Adam Malik MedangracedumaNoch keine Bewertungen
- SSEPDokument12 SeitenSSEPahippo100% (1)
- Tugas Stase Saraf Dr. AsriDokument37 SeitenTugas Stase Saraf Dr. Asriluthfianisa azhariNoch keine Bewertungen
- Feb 2015 - BJO - EMBRIOLOGY OF THE CNSDokument39 SeitenFeb 2015 - BJO - EMBRIOLOGY OF THE CNSihwan Ukhrawi AlyNoch keine Bewertungen
- Karakteristik Gangguan Tidur Pada Penyakit Parkinson Berdasarkan Parkinson Disease SleepDokument8 SeitenKarakteristik Gangguan Tidur Pada Penyakit Parkinson Berdasarkan Parkinson Disease SleepAfifa NingrumNoch keine Bewertungen
- CerebellumDokument62 SeitenCerebellumadelina.jianu9991Noch keine Bewertungen
- Deteksi Pre-Hospital StrokeDokument17 SeitenDeteksi Pre-Hospital StrokeDocApizzNoch keine Bewertungen
- Primary Headache in Clinical PracticeDokument68 SeitenPrimary Headache in Clinical PracticeAkbar RasyidsonyNoch keine Bewertungen
- Struktur Organisasi Neurologi 18 Mei 2020Dokument36 SeitenStruktur Organisasi Neurologi 18 Mei 2020MienaNoch keine Bewertungen
- DiensefalonDokument31 SeitenDiensefalonIngrid AykeNoch keine Bewertungen
- ASIA ScoreDokument2 SeitenASIA ScoreIqbal BaryarNoch keine Bewertungen
- Regeneration of Nervous SystemDokument37 SeitenRegeneration of Nervous SystemIdris LubisNoch keine Bewertungen
- Neurologi Klinis DasarklinicDokument19 SeitenNeurologi Klinis Dasarklinickloter1Noch keine Bewertungen
- Klasifikasi Tumor Paru Secara Histologis Menurut WHO Tahun 2015Dokument3 SeitenKlasifikasi Tumor Paru Secara Histologis Menurut WHO Tahun 2015lindaNoch keine Bewertungen
- Papilledema: Epidemiology, Etiology, and Clinical ManagementDokument11 SeitenPapilledema: Epidemiology, Etiology, and Clinical ManagementAita Utsukushi HyuugaNoch keine Bewertungen
- Ischialgia TraumatikDokument12 SeitenIschialgia TraumatikAnonymous qLL3HUgNoch keine Bewertungen
- Kuliah 3 - Tumor OtakDokument150 SeitenKuliah 3 - Tumor Otaktutorial. aNoch keine Bewertungen
- Cerebral Palsy: Causes and Treatment Alternatives, Based On The Evidence Provided by Gait Analysis - Rupcich M, Bravo RDokument2 SeitenCerebral Palsy: Causes and Treatment Alternatives, Based On The Evidence Provided by Gait Analysis - Rupcich M, Bravo RRicardo BravoNoch keine Bewertungen
- SyncopeDokument19 SeitenSyncopeIvana Ester Sinta UliNoch keine Bewertungen
- Neurogenic BladderDokument25 SeitenNeurogenic Bladderyouffa hanna elt misykahNoch keine Bewertungen
- Motor SystemDokument49 SeitenMotor SystemAhaisibwe GordonNoch keine Bewertungen
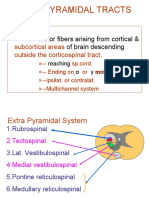
- Extrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingDokument21 SeitenExtrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingAsfoor gake1Noch keine Bewertungen
- NeuroTracts - Ascending, Descending, UMN, LMNDokument5 SeitenNeuroTracts - Ascending, Descending, UMN, LMNBrandi Allen HensonNoch keine Bewertungen
- DrMBA Medulla SpinalisDokument25 SeitenDrMBA Medulla SpinalisAyu FadhilahNoch keine Bewertungen
- HRCT Protocols & Artifacts: Leena. R. David M.SC - MITDokument24 SeitenHRCT Protocols & Artifacts: Leena. R. David M.SC - MITNadeem ShahNoch keine Bewertungen
- Objectives: Terms of Use Privacy Policy Notice AccessibilityDokument16 SeitenObjectives: Terms of Use Privacy Policy Notice AccessibilityJuan Sebas OspinaNoch keine Bewertungen
- Case Study: Ang Kwento Ni RosarioDokument2 SeitenCase Study: Ang Kwento Ni RosarioVerloren MorgensternNoch keine Bewertungen
- Parts of The Body and Health Problem Learning Objectives Students Should Be Able To Express The Location of The Pain in The Body VocabularyDokument13 SeitenParts of The Body and Health Problem Learning Objectives Students Should Be Able To Express The Location of The Pain in The Body VocabularySonia Tri AgustinaNoch keine Bewertungen
- 09 Marijuana Facts For TeensDokument24 Seiten09 Marijuana Facts For Teensapi-309082881Noch keine Bewertungen
- Logiq E10: Empowering You To Make A DifferenceDokument5 SeitenLogiq E10: Empowering You To Make A DifferenceMadalina C0% (1)
- Module 2 HistopathologyDokument34 SeitenModule 2 HistopathologyKim RuizNoch keine Bewertungen
- Acute Purulent Diseases of Fingers and HandDokument23 SeitenAcute Purulent Diseases of Fingers and Handluckyswiss7776848Noch keine Bewertungen
- Goat ManualDokument64 SeitenGoat ManualIrfan YaqoobNoch keine Bewertungen
- B1001A Practice Final Exam 2023Dokument15 SeitenB1001A Practice Final Exam 2023yeNoch keine Bewertungen
- SOSCG 6jul2013 v5Dokument32 SeitenSOSCG 6jul2013 v5Suhazeli Abdullah100% (2)
- DR Lie Khie Chen - Management of MDR Infection in Sepsis Jade 2016Dokument33 SeitenDR Lie Khie Chen - Management of MDR Infection in Sepsis Jade 2016Astria PermanaNoch keine Bewertungen
- Management of PPHDokument24 SeitenManagement of PPHMutabazi SharifNoch keine Bewertungen
- Msds Rheomax DR 1030 enDokument9 SeitenMsds Rheomax DR 1030 enBuenaventura Jose Huamani TalaveranoNoch keine Bewertungen
- Final 2016 ResumeDokument4 SeitenFinal 2016 Resumeapi-311457885Noch keine Bewertungen
- Msds PG LyondellDokument9 SeitenMsds PG LyondellGia Minh Tieu TuNoch keine Bewertungen
- DafpusDokument1 SeiteDafpusJeliny Bintan MaisuriNoch keine Bewertungen
- Refractory MigraineDokument495 SeitenRefractory MigraineSuresh Srinivas100% (1)
- Nej M CPC 2103461Dokument10 SeitenNej M CPC 2103461monaNoch keine Bewertungen
- Lesson Plan NutritionDokument7 SeitenLesson Plan NutritionPraveenNoch keine Bewertungen
- IvpbhandoutDokument2 SeitenIvpbhandoutapi-283303129Noch keine Bewertungen
- Immune Dysregulation Among Students Exposed To Exam Stress and Its Mitigation by Mindfulness Training - Findings From An Exploratory Randomised TrialDokument11 SeitenImmune Dysregulation Among Students Exposed To Exam Stress and Its Mitigation by Mindfulness Training - Findings From An Exploratory Randomised TrialPatricia Elena ManaliliNoch keine Bewertungen
- 2019 ACC AHA Guidelines For Primary Prevention of CV DiseaseDokument39 Seiten2019 ACC AHA Guidelines For Primary Prevention of CV DiseaseArdel RomeroNoch keine Bewertungen
- RS3772 - Grade - 9 Principle and Practices of Fruit Crop ProductionDokument96 SeitenRS3772 - Grade - 9 Principle and Practices of Fruit Crop ProductionMithlesh YadavNoch keine Bewertungen
- Biosimilar Approval ProcessDokument2 SeitenBiosimilar Approval ProcessMoustapha El-AmineNoch keine Bewertungen
- Using Master Tung's Gallbladder Points For Diseases of The Head and NeckDokument2 SeitenUsing Master Tung's Gallbladder Points For Diseases of The Head and NeckTrần Hồ Thạnh Phú100% (1)
- Antihypnotics and AnxiolyticsDokument12 SeitenAntihypnotics and AnxiolyticsSabreena NordinNoch keine Bewertungen
- Orthodontic Dental Casts The Case For Routine ArtiDokument8 SeitenOrthodontic Dental Casts The Case For Routine ArtiLuminous DentalNoch keine Bewertungen
- Volunteer Report FinalDokument11 SeitenVolunteer Report FinalBeenish JehangirNoch keine Bewertungen
- Fascial Fitness PDFDokument11 SeitenFascial Fitness PDFmari_kundera19Noch keine Bewertungen