Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
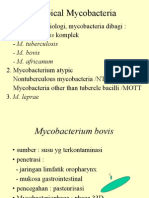
- Atypical Mycobacteria: DG Dasar Epidemiologi, Mycobacteria Dibagi: 1. M. Tuberculosis Komplek - M. TuberculosisDokument19 SeitenAtypical Mycobacteria: DG Dasar Epidemiologi, Mycobacteria Dibagi: 1. M. Tuberculosis Komplek - M. TuberculosisTiven StiveNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Electrolyte ImbalanceDokument44 SeitenElectrolyte ImbalanceTiven StiveNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Acute AppendisitisDokument27 SeitenAcute AppendisitisTiven StiveNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- SCAE Aicardi SyndromeDokument2 SeitenSCAE Aicardi SyndromeTiven StiveNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Diagnosis of Tension-Type Headache, Migraine and Cluster HeadacheDokument1 SeiteDiagnosis of Tension-Type Headache, Migraine and Cluster HeadacheTiven StiveNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- J2 P IntroductionDokument9 SeitenJ2 P IntroductionnitinvnjNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- E9d30c8 4837smartDokument1 SeiteE9d30c8 4837smartSantoshNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- YazdiDokument7 SeitenYazditrs1970Noch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- BoSY CRLA Grade 1 MT Administration GuideDokument13 SeitenBoSY CRLA Grade 1 MT Administration GuideJOCELYN SANANO100% (1)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Natural Gas DistributionDokument46 SeitenNatural Gas DistributionscribdmisraNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Effectives of e Wallets NewDokument15 SeitenEffectives of e Wallets NewRicardo SantosNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Fractal Blaster Trading Strategy ReportDokument22 SeitenFractal Blaster Trading Strategy ReportIcky IckyNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Regional Trial Court National Capital Judicial Region: ComplainantDokument5 SeitenRegional Trial Court National Capital Judicial Region: ComplainantNeil Patrick QuiniquiniNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Gurdan Saini: From Wikipedia, The Free EncyclopediaDokument6 SeitenGurdan Saini: From Wikipedia, The Free EncyclopediaRanjeet SinghNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Reich 0001 PDFDokument87 SeitenReich 0001 PDFYordys Domínguez RodríguezNoch keine Bewertungen
- Downtown SLO Business Owners Ask City Council To Consider Parking ChangesDokument4 SeitenDowntown SLO Business Owners Ask City Council To Consider Parking ChangesKaytlyn LeslieNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Urban Square Design: Landscape Design Studio III LAR 803Dokument44 SeitenUrban Square Design: Landscape Design Studio III LAR 803Peter DokpesiNoch keine Bewertungen
- Distribution IDokument28 SeitenDistribution IsruthiNoch keine Bewertungen
- Onechanbara - Bikini Samurai Squad Game GuideDokument83 SeitenOnechanbara - Bikini Samurai Squad Game GuideStefan RoscaNoch keine Bewertungen
- Pale ExamDokument4 SeitenPale ExamPatrick Tan100% (1)
- Milling Machine Maintenance, Safety and OperationDokument3 SeitenMilling Machine Maintenance, Safety and OperationPPSwain100% (1)
- Settlement Geography: Unit No-1&2Dokument11 SeitenSettlement Geography: Unit No-1&2Arindam RoulNoch keine Bewertungen
- Senate - Investigating - Committee - On - Education California Textbooks 1948 120pgs GOV EDU - SML PDFDokument115 SeitenSenate - Investigating - Committee - On - Education California Textbooks 1948 120pgs GOV EDU - SML PDFdragan346382902Noch keine Bewertungen
- 20 Heirs of Alfredo Bautista VS LindoDokument3 Seiten20 Heirs of Alfredo Bautista VS LindoJerome LeañoNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Sample Invoice PDFDokument3 SeitenSample Invoice PDFMarcus OlivieraaNoch keine Bewertungen
- Agne Vs Director of LandsDokument7 SeitenAgne Vs Director of LandsLee SomarNoch keine Bewertungen
- Apy1 Kinematics Review - 2015 - KeyDokument13 SeitenApy1 Kinematics Review - 2015 - KeyemadNoch keine Bewertungen
- Nocturne 2024Dokument162 SeitenNocturne 2024Peter JonesNoch keine Bewertungen
- Final Journal 2Dokument60 SeitenFinal Journal 2Swetha NikaljeNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Engineering Discourse Communities RMDokument4 SeitenEngineering Discourse Communities RMapi-336463296Noch keine Bewertungen
- Global Perspectives Reflective PaperDokument3 SeitenGlobal Perspectives Reflective PaperMoaiz AttiqNoch keine Bewertungen
- 1982 B47 Lehigh County Gunsmithing FamiliesDokument12 Seiten1982 B47 Lehigh County Gunsmithing FamiliesAmr DeabesNoch keine Bewertungen
- My Kindergarten BookDokument48 SeitenMy Kindergarten BookfranciscoNoch keine Bewertungen
- Markets and Commodity Figures: Total Market Turnover StatisticsDokument6 SeitenMarkets and Commodity Figures: Total Market Turnover StatisticsTiso Blackstar GroupNoch keine Bewertungen
- 1.4 Creating Graphic OrganizerDokument1 Seite1.4 Creating Graphic OrganizerTrixie Roselle Y. MesiasNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)