Das könnte Ihnen auch gefallen
- Chronic Renal FailureDokument14 SeitenChronic Renal FailureyazzzNoch keine Bewertungen
- Acute Liver FailureDokument3 SeitenAcute Liver FailureElisabeth F. OjhaNoch keine Bewertungen
- Renal Failur E: Mamta Kumari Asst - Prof. Igims-ConDokument51 SeitenRenal Failur E: Mamta Kumari Asst - Prof. Igims-ConMamta KumariNoch keine Bewertungen
- Diabetes Mellitus Complications GuideDokument48 SeitenDiabetes Mellitus Complications GuideAnditha Namira RS100% (1)
- Chronic Renal FailureDokument26 SeitenChronic Renal FailureRemington Thomas II100% (5)
- Chronic Kidney DiseaseDokument15 SeitenChronic Kidney Diseaseapi-270623039Noch keine Bewertungen
- Chronic Renal FailureDokument46 SeitenChronic Renal Failurestepharry08100% (1)
- Nursing Care of Acute Renal FailureDokument78 SeitenNursing Care of Acute Renal Failurejstrnad87100% (1)
- Mechanisms and Manifestations of Chronic Renal FailureDokument6 SeitenMechanisms and Manifestations of Chronic Renal FailureEmil GulmaticoNoch keine Bewertungen
- Nursing Care Plan for Aortic Aneurysm RepairDokument68 SeitenNursing Care Plan for Aortic Aneurysm RepairManila Prak100% (2)
- Acute Renal FailureDokument32 SeitenAcute Renal Failuresarguss14100% (5)
- Heart Failure With Preserved Ejection FractionDokument19 SeitenHeart Failure With Preserved Ejection Fractioncosmin balanNoch keine Bewertungen
- UROLITHIASISDokument9 SeitenUROLITHIASISmardsz100% (13)
- Cancer of The Colon and RectumDokument37 SeitenCancer of The Colon and Rectumapi-19641337100% (1)
- Chole CystDokument12 SeitenChole CystMoch NizamNoch keine Bewertungen
- Causes and Pathophysiology of Congestive Heart Failure (CHFDokument1 SeiteCauses and Pathophysiology of Congestive Heart Failure (CHFLance MarquezNoch keine Bewertungen
- Acute Renal FailureDokument13 SeitenAcute Renal FailureGlorianne Palor100% (2)
- Understanding the Pathophysiology of Coronary Artery DiseaseDokument14 SeitenUnderstanding the Pathophysiology of Coronary Artery DiseasejohnhenryvNoch keine Bewertungen
- Gastro Intestinal Bleeding DR - muayAD ABASSDokument59 SeitenGastro Intestinal Bleeding DR - muayAD ABASSMAFADHELNoch keine Bewertungen
- Pathophysiology of DMDokument4 SeitenPathophysiology of DMNicole Louise N. VillanuevaNoch keine Bewertungen
- Disorders of Small IntestineDokument41 SeitenDisorders of Small IntestineSamuel kuriaNoch keine Bewertungen
- Esophageal VaricesDokument14 SeitenEsophageal VaricesKarla So MejiaNoch keine Bewertungen
- Serum ElectrolytesDokument2 SeitenSerum ElectrolytesKervin CablaidaNoch keine Bewertungen
- Causes, Symptoms and Treatment of AtelectasisDokument4 SeitenCauses, Symptoms and Treatment of AtelectasisAshley Jane MacapayadNoch keine Bewertungen
- Liver CirrhosisDokument83 SeitenLiver CirrhosisRusiana NasilahNoch keine Bewertungen
- Lupus NephritisDokument15 SeitenLupus NephritisVilza maharaniNoch keine Bewertungen
- Urinary Tract InfectionDokument50 SeitenUrinary Tract Infectionpokhara gharipatanNoch keine Bewertungen
- Precautions With Diabetic Patients Undergoing SurgeryDokument6 SeitenPrecautions With Diabetic Patients Undergoing SurgeryErvin Kyle OsmeñaNoch keine Bewertungen
- CIRRHOSIS OF LIVER (Practice of Medicine)Dokument84 SeitenCIRRHOSIS OF LIVER (Practice of Medicine)simran kaurNoch keine Bewertungen
- Acute Renal Failure TeoriDokument24 SeitenAcute Renal Failure TeoriVera Andri YaniNoch keine Bewertungen
- UROLITHIASISDokument84 SeitenUROLITHIASISJheanAlphonsineT.MeansNoch keine Bewertungen
- Renal Failure and Kidney DiseaseDokument41 SeitenRenal Failure and Kidney Disease12046Noch keine Bewertungen
- Chronic Renal FailureDokument54 SeitenChronic Renal Failuresanjivdas100% (3)
- Obstructive Uropathy: Nitha. K 2 Year MSC NursingDokument67 SeitenObstructive Uropathy: Nitha. K 2 Year MSC NursingNITHA KNoch keine Bewertungen
- Dialyzer: by Daniel V Dialysis LecturerDokument52 SeitenDialyzer: by Daniel V Dialysis LecturerDani Dany100% (2)
- Cardiac Arrest CPR GuideDokument54 SeitenCardiac Arrest CPR GuideIdha FitriyaniNoch keine Bewertungen
- Biliary Tree LectureDokument58 SeitenBiliary Tree Lecturesgod34Noch keine Bewertungen
- Neurogenic ShockDokument11 SeitenNeurogenic Shocklulu voxNoch keine Bewertungen
- Jaundice: DR: Ramy A. SamyDokument42 SeitenJaundice: DR: Ramy A. Samyoscar3spurgeonNoch keine Bewertungen
- Cirrhosis of LiverDokument35 SeitenCirrhosis of LiverShazia Parveen100% (1)
- Nephrotic SyndromeDokument31 SeitenNephrotic Syndromedrhananfathy100% (1)
- Acute Renal FailureDokument35 SeitenAcute Renal FailureKaelyn Bello Giray100% (1)
- Septic ShockDokument16 SeitenSeptic ShockGelo JvrNoch keine Bewertungen
- Buerger DiseaseDokument3 SeitenBuerger DiseaseElmer DizonNoch keine Bewertungen
- AppendicitisDokument11 SeitenAppendicitisayuniNoch keine Bewertungen
- Renal Transplant ProtocolsDokument42 SeitenRenal Transplant ProtocolsParis VlachosNoch keine Bewertungen
- Bowel Obstruction Case StudyDokument11 SeitenBowel Obstruction Case StudyFatimah Batool NawazNoch keine Bewertungen
- Syndrome of Inapropriate Antidiuretic Hormone (SIADH)Dokument15 SeitenSyndrome of Inapropriate Antidiuretic Hormone (SIADH)Asrul Rahim100% (1)
- Antiphospholipid Syndrome and Pregnancy (Dengan Foto Punya DR RositaDokument9 SeitenAntiphospholipid Syndrome and Pregnancy (Dengan Foto Punya DR RositadidongNoch keine Bewertungen
- Acute Renal Failure: Dr. Bobi Ahmad S, S.KPDokument62 SeitenAcute Renal Failure: Dr. Bobi Ahmad S, S.KPdr.Bobi Ahmad Sahid, S.KepNoch keine Bewertungen
- CholecystitisDokument27 SeitenCholecystitisKadek Ariarta MahartamaNoch keine Bewertungen
- Case Presentation - CKDDokument27 SeitenCase Presentation - CKDAmanda Padma50% (2)
- HypertensionDokument8 SeitenHypertensiongilma100% (3)
- Acute Renal FailureDokument17 SeitenAcute Renal FailureAnitha SuprionoNoch keine Bewertungen
- Primary AldosteronismDokument31 SeitenPrimary AldosteronismSteph100% (1)
- Pulmonary EmbolismDokument4 SeitenPulmonary Embolismemmag1221100% (1)
- Pyelonephritis: Departemen Ilmu Penyakit Dalam FK Uii YogyakartaDokument33 SeitenPyelonephritis: Departemen Ilmu Penyakit Dalam FK Uii YogyakartaAndaru Tri Setyo WibowoNoch keine Bewertungen
- Urinary Stones DiseaseDokument40 SeitenUrinary Stones DiseaseRenaldy ThiorisNoch keine Bewertungen
- Pathogenesis and Management of Renal Failure and Replacement Therapy For Stage V Chronic Renal DiseaseDokument30 SeitenPathogenesis and Management of Renal Failure and Replacement Therapy For Stage V Chronic Renal DiseaseByzantine Wulandari ParubakNoch keine Bewertungen
- CKD in Children: Risk Factors, Stages, Complications & TreatmentDokument29 SeitenCKD in Children: Risk Factors, Stages, Complications & TreatmentAlvin OmondiNoch keine Bewertungen
- VIDAS Menu Jan 2016Dokument2 SeitenVIDAS Menu Jan 2016طلال الخولانيNoch keine Bewertungen
- Endocrine System ExamDokument4 SeitenEndocrine System ExamNirmala Josephine100% (1)
- l8 Cc2 Lab Hypothalamus and Pituitary Gland Wala Nahuman PoDokument15 Seitenl8 Cc2 Lab Hypothalamus and Pituitary Gland Wala Nahuman PoAlyanaNoch keine Bewertungen
- Cupping Therapy in InfertilityDokument46 SeitenCupping Therapy in Infertilitymrcyber75% (8)
- High Levels of Free TestosteroneDokument2 SeitenHigh Levels of Free TestosteroneADNoch keine Bewertungen
- Lyphochek Immunoassay Plus Control Levels 1, 2 and 3: Fecha de Revisión 2021-04-20 Indica Información RevisadaDokument25 SeitenLyphochek Immunoassay Plus Control Levels 1, 2 and 3: Fecha de Revisión 2021-04-20 Indica Información RevisadaMariam MangaNoch keine Bewertungen
- Human Male Reproductive SystemDokument45 SeitenHuman Male Reproductive Systemcyber secNoch keine Bewertungen
- Emulsification LipidsDokument23 SeitenEmulsification LipidsChard RINoch keine Bewertungen
- Endocrine HarmonyDokument68 SeitenEndocrine HarmonyafnanNoch keine Bewertungen
- Hormone Practice Test: StudentDokument17 SeitenHormone Practice Test: StudentKayne SuratosNoch keine Bewertungen
- 1.2 Reproductive Endocrinology (Lim)Dokument6 Seiten1.2 Reproductive Endocrinology (Lim)Jojo MendozaNoch keine Bewertungen
- Soal Tes ImpsqDokument3 SeitenSoal Tes ImpsqNandaNoch keine Bewertungen
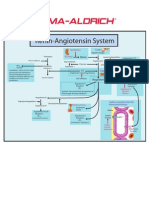
- Renin-Angiotensin SystemDokument1 SeiteRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Cushing-Syndrome SyndromeDokument16 SeitenCushing-Syndrome SyndromeVanetNoch keine Bewertungen
- Chapter 50: Nursing Management: Endocrine Problems Test BankDokument16 SeitenChapter 50: Nursing Management: Endocrine Problems Test BankPrince K. TaileyNoch keine Bewertungen
- Polycystic Ovarian Syndrome PPT 01Dokument50 SeitenPolycystic Ovarian Syndrome PPT 01Simone AquinoNoch keine Bewertungen
- Understanding Female Sexual AnatomyDokument90 SeitenUnderstanding Female Sexual AnatomyAndrea Monique R. Galasinao100% (1)
- Gannguan PubertasDokument56 SeitenGannguan PubertasAde Yosdi PutraNoch keine Bewertungen
- Assignment - Manuscript Review - 09012020Dokument5 SeitenAssignment - Manuscript Review - 09012020Nitya KrishnaNoch keine Bewertungen
- Journal Club - EichlerDokument4 SeitenJournal Club - Eichlerapi-648595816Noch keine Bewertungen
- CBE/BSE Exam QuestionsDokument8 SeitenCBE/BSE Exam QuestionsMay Chelle ErazoNoch keine Bewertungen
- PubertyDokument14 SeitenPubertyAdelle SmithNoch keine Bewertungen
- Accuracy of NIDDM Diagnosis Coding at Pertamina Jaya Hospital in 2016Dokument8 SeitenAccuracy of NIDDM Diagnosis Coding at Pertamina Jaya Hospital in 2016Yulia Putri RachmawatiNoch keine Bewertungen
- CH 01 Lecture PresentationDokument90 SeitenCH 01 Lecture PresentationNie TofuNoch keine Bewertungen
- Effect of Purwoceng Extract on Male Vitality Indicators in RatsDokument10 SeitenEffect of Purwoceng Extract on Male Vitality Indicators in RatsAnonymous HPmfOqdwNoch keine Bewertungen
- Causes, Types & Treatments of Breast Pain (MastalgiaDokument3 SeitenCauses, Types & Treatments of Breast Pain (MastalgiaColter Wallace CianoNoch keine Bewertungen
- DLC911 - Feedback Mechanism Lesson PlanDokument2 SeitenDLC911 - Feedback Mechanism Lesson PlanMariel CondesaNoch keine Bewertungen
- Case Study On: Lyceum of The Philippines UniversityDokument4 SeitenCase Study On: Lyceum of The Philippines UniversityarturogarcesjrNoch keine Bewertungen
- Sci10 LM U3Dokument131 SeitenSci10 LM U3Romel B Agno86% (7)
- Final Obstetrics and GynacologyDokument88 SeitenFinal Obstetrics and Gynacologysis8100% (2)