Das könnte Ihnen auch gefallen
- Preoperative Preparation of Patient For SurgeryDokument23 SeitenPreoperative Preparation of Patient For SurgeryFauzi SebunyaNoch keine Bewertungen
- Respiratory SystemDokument12 SeitenRespiratory SystemTricia CabiliNoch keine Bewertungen
- Asthma and CopdDokument44 SeitenAsthma and CopdBeer Dilacshe100% (1)
- Promoting Nutrition (Enteral Nutrition)Dokument51 SeitenPromoting Nutrition (Enteral Nutrition)Yayin Pestaño100% (1)
- Assignment On: Oxygen Administrration (Nasal Catheter, Mask, Oxygen Hood& Cpap)Dokument10 SeitenAssignment On: Oxygen Administrration (Nasal Catheter, Mask, Oxygen Hood& Cpap)Suganthi ParthibanNoch keine Bewertungen
- Ncp-Ineffective Airway ClearanceDokument3 SeitenNcp-Ineffective Airway Clearancelouanne0550% (2)
- Oxygen Therapy: by DR Finny Theo, MBBS, (DNB)Dokument59 SeitenOxygen Therapy: by DR Finny Theo, MBBS, (DNB)The Telugu DoctorNoch keine Bewertungen
- Nasogastric Tube Insertion: Nursing Guidelines and ConsiderationsDokument39 SeitenNasogastric Tube Insertion: Nursing Guidelines and ConsiderationsTiger KneeNoch keine Bewertungen
- Chest and LungsDokument49 SeitenChest and LungsChala KeneNoch keine Bewertungen
- Shock & Fluid TherapyDokument57 SeitenShock & Fluid Therapyarnol3090Noch keine Bewertungen
- Nclex review: Pneumonia, COPD, Asthma StudyDokument11 SeitenNclex review: Pneumonia, COPD, Asthma Studymj078Noch keine Bewertungen
- ChesttubedrainageDokument65 SeitenChesttubedrainagejerinthomasrajanNoch keine Bewertungen
- NCP Impaired Gas ExchangeDokument2 SeitenNCP Impaired Gas ExchangeCharissa Magistrado De LeonNoch keine Bewertungen
- SuctioningDokument30 SeitenSuctioningbajaoc60% (5)
- Mechanical Ventilation 8.2.17Dokument41 SeitenMechanical Ventilation 8.2.17SyafiqAziziNoch keine Bewertungen
- Pneumonia: DefinitionDokument5 SeitenPneumonia: DefinitionhemaanandhyNoch keine Bewertungen
- Mechanical Ventilator Management ProtocolDokument3 SeitenMechanical Ventilator Management ProtocolRick Frea100% (2)
- Modes of Mechanical Ventilation GuideDokument34 SeitenModes of Mechanical Ventilation Guidesbraj86100% (1)
- Form 3 Chapter 1 QuestionsDokument11 SeitenForm 3 Chapter 1 QuestionsCheah Foo Kit50% (2)
- Viral Exanthem (Main)Dokument94 SeitenViral Exanthem (Main)Starlet Rhonadez Bito-onon OrielNoch keine Bewertungen
- LungspatternDokument15 SeitenLungspatternquehacesmadridNoch keine Bewertungen
- Procedure 48-4: Suctioning A Tracheostomy or Endotracheal TubeDokument4 SeitenProcedure 48-4: Suctioning A Tracheostomy or Endotracheal Tubeamal abdulrahmanNoch keine Bewertungen
- 118 Skills Lab-Week 1-Responses To Altered Ventilatory FunctionsDokument8 Seiten118 Skills Lab-Week 1-Responses To Altered Ventilatory FunctionsKeisha BartolataNoch keine Bewertungen
- Opioid Analgesics & Antagonists: Dr. Hayder B Sahib Ph.D. PharmacologyDokument47 SeitenOpioid Analgesics & Antagonists: Dr. Hayder B Sahib Ph.D. Pharmacologyarham pirachaNoch keine Bewertungen
- Oxygenation QuizDokument3 SeitenOxygenation QuizPOTENCIANA MAROMANoch keine Bewertungen
- Breathing System: Assembly and Functional Analysis: DR Ashutosh Verma Moderator-Dr ChetnaDokument79 SeitenBreathing System: Assembly and Functional Analysis: DR Ashutosh Verma Moderator-Dr Chetnaaahutosh vermaNoch keine Bewertungen
- Uses of Inhaler DevicesDokument39 SeitenUses of Inhaler Devicesluis_chubeeNoch keine Bewertungen
- 780 Adult Cardio Resp Assess DSTDokument10 Seiten780 Adult Cardio Resp Assess DSTGursangeet Kaur100% (1)
- Asthma (Reactive Airway Disease)Dokument33 SeitenAsthma (Reactive Airway Disease)anwar jabariNoch keine Bewertungen
- Oxygen Therapy: Administration and SafetyDokument21 SeitenOxygen Therapy: Administration and SafetyGeraldine MaeNoch keine Bewertungen
- Diagnosis & Treament: ShockDokument52 SeitenDiagnosis & Treament: ShockasepNoch keine Bewertungen
- Administration of O2 TherapyDokument36 SeitenAdministration of O2 TherapyFatima Ysabelle Marie RuizNoch keine Bewertungen
- Causes and Treatment of EpistaxisDokument40 SeitenCauses and Treatment of EpistaxisSilar KhanNoch keine Bewertungen
- Types of InhalersDokument23 SeitenTypes of Inhalersshamie1110Noch keine Bewertungen
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesVon EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNoch keine Bewertungen
- Expanded Program On ImmunizationDokument23 SeitenExpanded Program On ImmunizationKate E. GatchalianNoch keine Bewertungen
- Umbilical Artery Catheterization for Blood Pressure MonitoringDokument11 SeitenUmbilical Artery Catheterization for Blood Pressure MonitoringRhaq Sheldon-CoelhoNoch keine Bewertungen
- Barangay Health Governance Body 2018Dokument44 SeitenBarangay Health Governance Body 2018Donna Lei G. RosarioNoch keine Bewertungen
- NSG 117 PerfusionDokument55 SeitenNSG 117 PerfusionAnonymous UJEyEsNoch keine Bewertungen
- Nursing Care PlanDokument14 SeitenNursing Care PlanVin Landicho100% (1)
- Degenerative Disease of CNSDokument50 SeitenDegenerative Disease of CNSRadhikaNoch keine Bewertungen
- Sister Kuan ExplanationDokument7 SeitenSister Kuan Explanationluis_chubee100% (2)
- Tracheostomy Procedure ExplainedDokument6 SeitenTracheostomy Procedure ExplainedMa. Ydela Meradores100% (1)
- IntubationDokument41 SeitenIntubationNice YouNoch keine Bewertungen
- Seminar Asthma PDFDokument39 SeitenSeminar Asthma PDFAriff Mahdzub0% (1)
- Shock ManagementDokument45 SeitenShock ManagementJean Gwyneth GatchalianNoch keine Bewertungen
- Antiretroviral Therapy: Awlachew Firde (S.Pharmacist)Dokument40 SeitenAntiretroviral Therapy: Awlachew Firde (S.Pharmacist)wedajoyonas50Noch keine Bewertungen
- OxygenationDokument57 SeitenOxygenationassumptaNoch keine Bewertungen
- ARDSDokument27 SeitenARDSChloie Marie RosalejosNoch keine Bewertungen
- Respiration 16 Respiratory FailureDokument31 SeitenRespiration 16 Respiratory Failureapi-19641337Noch keine Bewertungen
- DiphtheriaDokument22 SeitenDiphtheriaLovely Acabado TampocoNoch keine Bewertungen
- Infectious Disease Medications ModuleDokument8 SeitenInfectious Disease Medications ModuleSheril MarekNoch keine Bewertungen
- Mechanical Ventilation and Intracranial PressureDokument30 SeitenMechanical Ventilation and Intracranial PressureFlavius AnghelNoch keine Bewertungen
- Oxygenation NCM 103Dokument10 SeitenOxygenation NCM 103Richmond LacadenNoch keine Bewertungen
- CopdDokument14 SeitenCopdMohd Farid Bin RosliNoch keine Bewertungen
- NCM100 Cystoclysis CareDokument2 SeitenNCM100 Cystoclysis CarecchiechieNoch keine Bewertungen
- 161111163114Dokument31 Seiten161111163114lejizixNoch keine Bewertungen
- Oxygen Delivery Devices: Dr. HimanshuDokument40 SeitenOxygen Delivery Devices: Dr. HimanshusnezaimNoch keine Bewertungen
- Poisoning DecontaminationDokument14 SeitenPoisoning DecontaminationadystiNoch keine Bewertungen
- Respiratory Failure PresentationDokument13 SeitenRespiratory Failure PresentationHusnain Irshad AlviNoch keine Bewertungen
- Lower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDokument95 SeitenLower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingRI NANoch keine Bewertungen
- 10 AsthmaDokument39 Seiten10 AsthmaAkash MishraNoch keine Bewertungen
- Aerosol Therapy TMK 1Dokument34 SeitenAerosol Therapy TMK 1Inna DoroshkevychNoch keine Bewertungen
- Aerosoltherapy Nebu 120503115712 Phpapp01Dokument65 SeitenAerosoltherapy Nebu 120503115712 Phpapp01Aan Ika SugathotNoch keine Bewertungen
- Respiratory Care ModalitiesDokument63 SeitenRespiratory Care ModalitiesErica Clerigo LandichoNoch keine Bewertungen
- OxygenationDokument50 SeitenOxygenationLulu MushiNoch keine Bewertungen
- Women's Pneumonia ReportDokument9 SeitenWomen's Pneumonia ReportNohaira SADANGNoch keine Bewertungen
- Respiratory Failure Nursing Care and ManagementDokument19 SeitenRespiratory Failure Nursing Care and ManagementYudionoNoch keine Bewertungen
- Pediatric Lung Diseases: Empyema and Lung AbscessDokument39 SeitenPediatric Lung Diseases: Empyema and Lung AbscessFaisal MoidunnyNoch keine Bewertungen
- TracheostomyDokument28 SeitenTracheostomyprivatejarjarbinksNoch keine Bewertungen
- Tracheostomy Procedure GuideDokument18 SeitenTracheostomy Procedure GuideSudhanshu ShekharNoch keine Bewertungen
- Procedure Checklist On Tracheostomy CareDokument2 SeitenProcedure Checklist On Tracheostomy CareDoc Zay VillafuerteNoch keine Bewertungen
- Communicable DiseasesDokument24 SeitenCommunicable DiseasesJanus de LeonNoch keine Bewertungen
- Sister Letty G. Kuan: "Retirement and Role Discontinuities"Dokument25 SeitenSister Letty G. Kuan: "Retirement and Role Discontinuities"luis_chubeeNoch keine Bewertungen
- SGD GrossDokument10 SeitenSGD Grossluis_chubeeNoch keine Bewertungen
- SGD Gross AnatomyDokument11 SeitenSGD Gross Anatomyluis_chubeeNoch keine Bewertungen
- NeedlestickDokument14 SeitenNeedlestickluis_chubeeNoch keine Bewertungen
- Triage in Mass Casualty IncidentsDokument55 SeitenTriage in Mass Casualty Incidentsluis_chubeeNoch keine Bewertungen
- Needle Stick Injury CaseDokument5 SeitenNeedle Stick Injury Caseluis_chubeeNoch keine Bewertungen
- Client PresentationDokument4 SeitenClient Presentationluis_chubeeNoch keine Bewertungen
- Micro SGDDokument13 SeitenMicro SGDluis_chubeeNoch keine Bewertungen
- Respiratory SystemDokument29 SeitenRespiratory Systemluis_chubeeNoch keine Bewertungen
- 10 Gloden Rules in Administering Drug SafelyDokument4 Seiten10 Gloden Rules in Administering Drug Safelyluis_chubeeNoch keine Bewertungen
- 10 Gloden Rules in Administering Drug SafelyDokument4 Seiten10 Gloden Rules in Administering Drug Safelyluis_chubeeNoch keine Bewertungen
- I. Clinical QuestionDokument3 SeitenI. Clinical Questionluis_chubeeNoch keine Bewertungen
- Pathophysiology of Pulmonary Tuberculosis PTBDokument1 SeitePathophysiology of Pulmonary Tuberculosis PTBluis_chubeeNoch keine Bewertungen
- SGD PediaDokument12 SeitenSGD Pedialuis_chubeeNoch keine Bewertungen
- Ecologic ModelDokument2 SeitenEcologic Modelluis_chubeeNoch keine Bewertungen
- Branches and Differences of PhoneticsDokument4 SeitenBranches and Differences of Phoneticsmaryjames ikebunaNoch keine Bewertungen
- Mechanics of Breathiq H Man': He Mechanical WorkDokument16 SeitenMechanics of Breathiq H Man': He Mechanical WorkZOUAQ KarimNoch keine Bewertungen
- Pulmonary Function Tests (PFT)Dokument30 SeitenPulmonary Function Tests (PFT)براءة أحمد السلاماتNoch keine Bewertungen
- The Respiratory System: SubtitleDokument89 SeitenThe Respiratory System: SubtitleAaaNoch keine Bewertungen
- Edit NG Drug StudyDokument35 SeitenEdit NG Drug StudyAlleinad BarracasNoch keine Bewertungen
- Nurse sees post-op appendectomy client first after endorsementDokument9 SeitenNurse sees post-op appendectomy client first after endorsementMishia Renee EchonNoch keine Bewertungen
- Test Bank For Respiratory Disease A Case Study Approach To Patient Care 3rd Edition WilkinsDokument36 SeitenTest Bank For Respiratory Disease A Case Study Approach To Patient Care 3rd Edition Wilkinscreutzerpilement1x24a100% (34)
- Factors Affecting Lung FunctionDokument6 SeitenFactors Affecting Lung FunctionVia GallagherNoch keine Bewertungen
- URTIDokument2 SeitenURTIYogeshRavalNoch keine Bewertungen
- 05.12 Anatomy of The Larynx & Physiology of PhonationDokument30 Seiten05.12 Anatomy of The Larynx & Physiology of PhonationReg LagartejaNoch keine Bewertungen
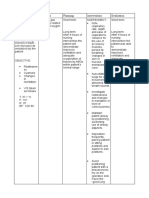
- Epiglottitis: Assessment Nursing Diagnosis Scientific Explanatio N Planning Nursing Intervention Rationale EvaluationDokument3 SeitenEpiglottitis: Assessment Nursing Diagnosis Scientific Explanatio N Planning Nursing Intervention Rationale EvaluationfifiNoch keine Bewertungen
- DLL Science-6 Q2 W2Dokument5 SeitenDLL Science-6 Q2 W2Ma Catherine Villanueva100% (1)
- XrayDokument106 SeitenXrayRaine BowNoch keine Bewertungen
- Life Processes XDokument124 SeitenLife Processes XAyush SinghNoch keine Bewertungen
- Design and Simulation of Mechanical VentilatorsDokument13 SeitenDesign and Simulation of Mechanical VentilatorsRaghavNoch keine Bewertungen
- A Collapsed Lung at 2Dokument22 SeitenA Collapsed Lung at 2Ryuina_sea05Noch keine Bewertungen
- Test Bank Chapter 26: Nursing Assessment: Respiratory SystemDokument11 SeitenTest Bank Chapter 26: Nursing Assessment: Respiratory SystemBriseidaSolisNoch keine Bewertungen
- 1 Label The Diagram Below.: Chapter 1: RespirationDokument10 Seiten1 Label The Diagram Below.: Chapter 1: RespirationNuzul HaikalNoch keine Bewertungen
- Circulatory and Respiratory System, Working TogetherDokument32 SeitenCirculatory and Respiratory System, Working TogetherRhona AngelaNoch keine Bewertungen
- A&P 302 - Respiratory NotesDokument31 SeitenA&P 302 - Respiratory NotesBethanyNoch keine Bewertungen