Das könnte Ihnen auch gefallen
- Maxillary Anesthetic TechniquesDokument83 SeitenMaxillary Anesthetic TechniquesAnonymous k8rDEsJsU1Noch keine Bewertungen
- Step by Step Root Canal Treatment PDFDokument156 SeitenStep by Step Root Canal Treatment PDFioana373280% (10)
- Extraction PDFDokument8 SeitenExtraction PDFAnonymous k8rDEsJsU1Noch keine Bewertungen
- Endo Perio LesionsDokument7 SeitenEndo Perio LesionsAnonymous k8rDEsJsU1Noch keine Bewertungen
- Intraoral RadiographyDokument18 SeitenIntraoral RadiographyAnonymous k8rDEsJsU10% (1)
- Neural Control of MasticationDokument34 SeitenNeural Control of MasticationAnonymous k8rDEsJsU10% (1)
- Nitrous Oxide Sedation DentistryDokument16 SeitenNitrous Oxide Sedation DentistryAnonymous k8rDEsJsU1100% (1)
- Common Oral Lesions: by Joseph Knight, PA-CDokument7 SeitenCommon Oral Lesions: by Joseph Knight, PA-CAnonymous k8rDEsJsU1Noch keine Bewertungen
- Basic Periodontal ExamDokument3 SeitenBasic Periodontal ExamAnonymous k8rDEsJsU1Noch keine Bewertungen
- Oral Health and HIV Disease: Carol M. Stewart DDS, MSDokument60 SeitenOral Health and HIV Disease: Carol M. Stewart DDS, MSAnonymous k8rDEsJsU1Noch keine Bewertungen
- Full Metal Crown ConstructionDokument48 SeitenFull Metal Crown ConstructionAnonymous k8rDEsJsU1100% (1)
- The SkullDokument123 SeitenThe SkullAnonymous k8rDEsJsU1Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Introduction To Endocrinology For Clinical StudentsDokument9 SeitenIntroduction To Endocrinology For Clinical StudentsOhwovoriole ToketemuNoch keine Bewertungen
- Diagnosis and Treatment of Vulvar Precancerous Lesions and CancerDokument4 SeitenDiagnosis and Treatment of Vulvar Precancerous Lesions and CancerSyahril FauziNoch keine Bewertungen
- Kidney HistogenesisDokument9 SeitenKidney HistogenesisKshitija KasturiNoch keine Bewertungen
- Non-Invasive Prenatal Testing (NIPT)Dokument13 SeitenNon-Invasive Prenatal Testing (NIPT)Andy WijayaNoch keine Bewertungen
- PDF Edexcel Biology Unit 1 Model Answers As Level - Compress PDFDokument2 SeitenPDF Edexcel Biology Unit 1 Model Answers As Level - Compress PDFsaadNoch keine Bewertungen
- Management of Deep Carious LesionsDokument5 SeitenManagement of Deep Carious LesionsEmeka V. ObiNoch keine Bewertungen
- Biological Effects of RadiationDokument28 SeitenBiological Effects of Radiationk_472894540Noch keine Bewertungen
- Atezolizumab For First-Line Treatment of Metastatic Nonsquamous NSCLCDokument14 SeitenAtezolizumab For First-Line Treatment of Metastatic Nonsquamous NSCLCMr. LNoch keine Bewertungen
- American Board of Prostodontics 2007Dokument52 SeitenAmerican Board of Prostodontics 2007Roberto Puc100% (2)
- PsychologyDokument55 SeitenPsychologyMukeshNoch keine Bewertungen
- Overview of The Classification and Treatment of Rapidly Progressive (Crescentic) GlomerulonephritisDokument6 SeitenOverview of The Classification and Treatment of Rapidly Progressive (Crescentic) GlomerulonephritisMarta AlberolaNoch keine Bewertungen
- Grade 8 Science 3rd QuarterDokument2 SeitenGrade 8 Science 3rd QuarterKeanu Ribs80% (30)
- Challis, Debbie The Archaeology of Race The Eugenic Ideas of FrancisDokument217 SeitenChallis, Debbie The Archaeology of Race The Eugenic Ideas of FrancisSonicoNoch keine Bewertungen
- Colony MorphologyDokument9 SeitenColony MorphologyKirk AdderleyNoch keine Bewertungen
- Clinical Practice Guideline For Management For Rehabilitation of Lower Limb AmputationDokument55 SeitenClinical Practice Guideline For Management For Rehabilitation of Lower Limb Amputationburtyx100% (1)
- Hester-Biosciences Karvy 010915 PDFDokument17 SeitenHester-Biosciences Karvy 010915 PDFmannimanojNoch keine Bewertungen
- Topic 3.4 WorksheetDokument5 SeitenTopic 3.4 WorksheetYixuan PENGNoch keine Bewertungen
- Roche GlucoseDokument4 SeitenRoche GlucoseDiep LeNoch keine Bewertungen
- What Is Sleep Paralysis ?Dokument7 SeitenWhat Is Sleep Paralysis ?Alle LOBSNoch keine Bewertungen
- 9 SC TissueDokument8 Seiten9 SC Tissuevishesh1997Noch keine Bewertungen
- Diagnostic Criteria For The Behavioral Variant FTDDokument5 SeitenDiagnostic Criteria For The Behavioral Variant FTDMusleh AlgarniNoch keine Bewertungen
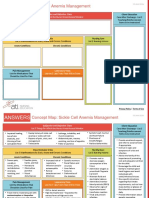
- NCC-SickleCellAnemiaManagement ConceptMap InteractivePDFDokument2 SeitenNCC-SickleCellAnemiaManagement ConceptMap InteractivePDFLoggerz Arck100% (1)
- 1.3 Studying LifeDokument7 Seiten1.3 Studying LifeDhani FajarNoch keine Bewertungen
- The EBC 46 Cancer TreatmentDokument9 SeitenThe EBC 46 Cancer TreatmentAnimefan TheoNoch keine Bewertungen
- P58450a Sa Ial Biology Wbi05 01 Oct19 6th ProofDokument8 SeitenP58450a Sa Ial Biology Wbi05 01 Oct19 6th ProofImran MushtaqNoch keine Bewertungen
- Antibiotic Resistance: Can We Ever Win?: Case Study BiologyDokument5 SeitenAntibiotic Resistance: Can We Ever Win?: Case Study Biologypabloandres zaratemarroquinNoch keine Bewertungen
- 21: Bone Wound Healing and OsseointegrationDokument15 Seiten21: Bone Wound Healing and OsseointegrationNYUCD17Noch keine Bewertungen
- Name Permanent Address Phone E-Mail Date of Birth Age Sex Religion Nationality Languages Known Academic DetailsDokument4 SeitenName Permanent Address Phone E-Mail Date of Birth Age Sex Religion Nationality Languages Known Academic DetailsrachanananoNoch keine Bewertungen
- Dr. Claude Negrier KOL Adult Hematologist France 112112 - TEMPLATEDokument10 SeitenDr. Claude Negrier KOL Adult Hematologist France 112112 - TEMPLATESOUMANLALANoch keine Bewertungen
- Medical NuggetsDokument8 SeitenMedical NuggetsDrGandhi Bhaskar Patrudu LankaNoch keine Bewertungen