Das könnte Ihnen auch gefallen
- To Perforasi GasterDokument27 SeitenTo Perforasi GasterPuthu BelegugNoch keine Bewertungen
- CCDuodenum Periampullary Neoplasms ChuDokument68 SeitenCCDuodenum Periampullary Neoplasms ChuSahirNoch keine Bewertungen
- Scalp Flaps & Craniotomy PrinciplesDokument41 SeitenScalp Flaps & Craniotomy PrinciplesKaramsi Gopinath NaikNoch keine Bewertungen
- Av Shunt PPDokument34 SeitenAv Shunt PPwahyuartyningsihNoch keine Bewertungen
- Discuss Thoracic IncisionsDokument47 SeitenDiscuss Thoracic IncisionsSucipto HartonoNoch keine Bewertungen
- Chronic Limb IschemiaDokument29 SeitenChronic Limb IschemiaSadia NaveedNoch keine Bewertungen
- Kompartemen SindromDokument9 SeitenKompartemen SindromPutri PratiwiNoch keine Bewertungen
- Pande Komang Gerry Paramesta: Decision Making in Bowel Obstruction: A Review byDokument32 SeitenPande Komang Gerry Paramesta: Decision Making in Bowel Obstruction: A Review byanon_550250832100% (1)
- Current Diagnosis and Management of Hirschsprung's DiseaseDokument20 SeitenCurrent Diagnosis and Management of Hirschsprung's DiseaseIyan AsianaNoch keine Bewertungen
- Wound de His Cence FinalDokument26 SeitenWound de His Cence Finaldanil armandNoch keine Bewertungen
- BPHDokument10 SeitenBPHMichelle SalimNoch keine Bewertungen
- Tg13: Updated Tokyo Guidelinesfor Acute CholecystitisDokument59 SeitenTg13: Updated Tokyo Guidelinesfor Acute CholecystitisDeoValendraNoch keine Bewertungen
- Teknik Operasi Splenektomi 2Dokument31 SeitenTeknik Operasi Splenektomi 2sphericalfaNoch keine Bewertungen
- Arch Bar and Ernst Ligature for Mandibular Fracture FixationDokument28 SeitenArch Bar and Ernst Ligature for Mandibular Fracture FixationFachrul Latif DentistNoch keine Bewertungen
- Jurnal Tyroid PDFDokument3 SeitenJurnal Tyroid PDFVinnaNoch keine Bewertungen
- LONG CASE Luka BakarDokument16 SeitenLONG CASE Luka BakarAfiazka LuthfitaNoch keine Bewertungen
- Xanthogranulomatous PyelonephritisDokument14 SeitenXanthogranulomatous PyelonephritisalaaNoch keine Bewertungen
- Slide Perbedaan Appendicitis Akut, Appendicitis Infiltrat Dan AbsesDokument30 SeitenSlide Perbedaan Appendicitis Akut, Appendicitis Infiltrat Dan AbsesJessica Giovanni RuntuNoch keine Bewertungen
- Colonic Volvulus RadiologyDokument25 SeitenColonic Volvulus RadiologyDhea Faizia TasyaNoch keine Bewertungen
- Diagnostic Peritoneal Lavage (DPL)Dokument10 SeitenDiagnostic Peritoneal Lavage (DPL)hatem alsrour100% (2)
- FlapDokument4 SeitenFlapMd Ahsanuzzaman PinkuNoch keine Bewertungen
- Chronic Limb Threatening IschemiaDokument35 SeitenChronic Limb Threatening Ischemiasifatullah khanNoch keine Bewertungen
- Diaphragma InjuryDokument18 SeitenDiaphragma InjuryAhmedNoch keine Bewertungen
- AdhesiolisisDokument22 SeitenAdhesiolisisRisal WintokoNoch keine Bewertungen
- Acute Abdomen and PeritonitisDokument17 SeitenAcute Abdomen and PeritonitisAnisaPratiwiArumningsihNoch keine Bewertungen
- Management of Urethral StricturesDokument5 SeitenManagement of Urethral StricturesYohana Elisabeth GultomNoch keine Bewertungen
- Herniotomy Procedure and Inguinal Canal AnatomyDokument16 SeitenHerniotomy Procedure and Inguinal Canal AnatomykawaishoneNoch keine Bewertungen
- Chest Tube Insertion GuideDokument8 SeitenChest Tube Insertion GuideTaufik Nur YahyaNoch keine Bewertungen
- Wound Healing Normal and Abnormal Mechanisms and Closure TechniquesDokument40 SeitenWound Healing Normal and Abnormal Mechanisms and Closure TechniquesAhmad Fakhrozi Helmi100% (1)
- Tracheostomy Procedure GuideDokument10 SeitenTracheostomy Procedure GuideAinur AbdrakhmanovaNoch keine Bewertungen
- Fracture and Dislocation-Rahardyan Magetsari (2016) PDFDokument105 SeitenFracture and Dislocation-Rahardyan Magetsari (2016) PDFRobertOktaChandraNoch keine Bewertungen
- ANATOMI ColorectalDokument16 SeitenANATOMI ColorectalShannonCPMNoch keine Bewertungen
- ROZERPLASTYDokument13 SeitenROZERPLASTYSaraya AmajidaNoch keine Bewertungen
- CA MammaeDokument30 SeitenCA MammaeAlfiany SahrNoch keine Bewertungen
- Thoracotomy ProcedureDokument19 SeitenThoracotomy ProceduresphericalfaNoch keine Bewertungen
- OsteosarkomaDokument2 SeitenOsteosarkomaLinawati DLNoch keine Bewertungen
- 2013 - Pancreaticoduodenectomy (Whipple Procedure) TechniquesDokument11 Seiten2013 - Pancreaticoduodenectomy (Whipple Procedure) TechniquesOlteanu IonutNoch keine Bewertungen
- Disorders of Epiphyseal Growth and DevelopmentDokument64 SeitenDisorders of Epiphyseal Growth and DevelopmentFebee NathaliaNoch keine Bewertungen
- Acute Pancreatitis: Methas Arunnart MD. Songkhla HospitalDokument70 SeitenAcute Pancreatitis: Methas Arunnart MD. Songkhla HospitalMohd ImranNoch keine Bewertungen
- Overgranulation: A. Muhammad Reva A.MDokument21 SeitenOvergranulation: A. Muhammad Reva A.Mgalih widodoNoch keine Bewertungen
- Vovulusoriginal Copy 121028055752 Phpapp01Dokument37 SeitenVovulusoriginal Copy 121028055752 Phpapp01Bheru LalNoch keine Bewertungen
- Tension Pneumothorax by AnkurDokument30 SeitenTension Pneumothorax by AnkurAnkur AgrawalNoch keine Bewertungen
- Surgery of PancreasDokument30 SeitenSurgery of PancreasmackieccNoch keine Bewertungen
- Ivc InjuryDokument17 SeitenIvc InjuryAnishChowdhuryNoch keine Bewertungen
- Jurnal CA TyroidDokument4 SeitenJurnal CA TyroidErvina ZelfiNoch keine Bewertungen
- Duodenal InjuryDokument54 SeitenDuodenal InjuryTony HardianNoch keine Bewertungen
- Systemic Therapies of CRC: Johan KurniandaDokument56 SeitenSystemic Therapies of CRC: Johan KurniandaANISA RACHMITA ARIANTI 2020Noch keine Bewertungen
- Guidelines for Resuscitation of Sepsis: Early Goals-Directed Therapy (EGDTDokument8 SeitenGuidelines for Resuscitation of Sepsis: Early Goals-Directed Therapy (EGDTsiti fatmalaNoch keine Bewertungen
- Retractile Testis PDFDokument6 SeitenRetractile Testis PDFDella Elvina RoeslandNoch keine Bewertungen
- Hernia World Conference ProgramDokument112 SeitenHernia World Conference ProgramYovan Prakosa100% (1)
- MESSDokument9 SeitenMESStaufik sofistiawanNoch keine Bewertungen
- Acute AbdomenDokument42 SeitenAcute AbdomenErika Agustina KasdjonoNoch keine Bewertungen
- WoundDokument38 SeitenWoundTaufiq HidayatNoch keine Bewertungen
- Gastric Perforation in The Newborn: Ai-Xuan Le Holterman, M.DDokument23 SeitenGastric Perforation in The Newborn: Ai-Xuan Le Holterman, M.Dpldhy2004Noch keine Bewertungen
- HerniaDokument61 SeitenHerniaAhmed HassanNoch keine Bewertungen
- Tenosynovitis Treatment and DiagnosisDokument32 SeitenTenosynovitis Treatment and DiagnosissultantraNoch keine Bewertungen
- Sitogenetika&variasi GenetikDokument147 SeitenSitogenetika&variasi GenetikDiniNoch keine Bewertungen
- Cotton and Williams' Practical Gastrointestinal Endoscopy: The FundamentalsVon EverandCotton and Williams' Practical Gastrointestinal Endoscopy: The FundamentalsNoch keine Bewertungen
- Dermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaVon EverandDermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaNoch keine Bewertungen
- Esophageal Motility Disorders and Gastroesophageal Reflux DiseaseDokument12 SeitenEsophageal Motility Disorders and Gastroesophageal Reflux DiseaseJuan JoseNoch keine Bewertungen
- Digestive SystemDokument6 SeitenDigestive SystemCeleste Atienza BawagNoch keine Bewertungen
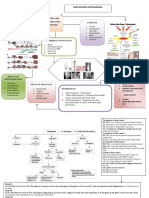
- Patogenesis RA SKEMADokument2 SeitenPatogenesis RA SKEMAAyu Rahmi AMyNoch keine Bewertungen
- In Vivo Studies of Mechanical Stress Effects On IVD Have BeenDokument1 SeiteIn Vivo Studies of Mechanical Stress Effects On IVD Have BeenJuanNoch keine Bewertungen
- Harmening Chapter Summary and Questions CompilationDokument63 SeitenHarmening Chapter Summary and Questions CompilationShaira Rae BillenaNoch keine Bewertungen
- Anatomy and Physiology of the Digestive SystemDokument9 SeitenAnatomy and Physiology of the Digestive SystemSamer SumalinogNoch keine Bewertungen
- Pulmo Management Week 1Dokument160 SeitenPulmo Management Week 1Dharlyn MungcalNoch keine Bewertungen
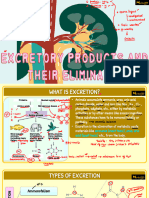
- Vipin Sir Biology 19. Excretory Products and Their EliminationDokument55 SeitenVipin Sir Biology 19. Excretory Products and Their EliminationvanshpatelssisNoch keine Bewertungen
- Unit XDokument18 SeitenUnit XPreeti ChouhanNoch keine Bewertungen
- Cambridge International AS & A Level: Biology 9700/23 October/November 2020Dokument20 SeitenCambridge International AS & A Level: Biology 9700/23 October/November 2020Vinayak KhedekarNoch keine Bewertungen
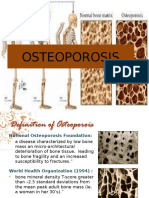
- OsteoporosisDokument13 SeitenOsteoporosisMimi Suhaini SudinNoch keine Bewertungen
- Ishihara2018 Barret JaponesDokument9 SeitenIshihara2018 Barret JaponesBety Puma PauccaraNoch keine Bewertungen
- CSB337 Trauma Study Guide QuestionsDokument36 SeitenCSB337 Trauma Study Guide QuestionsTessNoch keine Bewertungen
- Anatomy of The GI TractDokument174 SeitenAnatomy of The GI TractBenjamin Prabhu100% (1)
- Essentials of Anatomy & Physiology Chapter 4 Epithelial TissueDokument12 SeitenEssentials of Anatomy & Physiology Chapter 4 Epithelial TissueCASSANDRA BARQUILLANoch keine Bewertungen
- Cambridge IGCSE: Biology 0610/22Dokument16 SeitenCambridge IGCSE: Biology 0610/22Aisha YousifNoch keine Bewertungen
- Life Process Chapter QuestionsDokument11 SeitenLife Process Chapter QuestionsAdwaith TsNoch keine Bewertungen
- 7th Grade Shrimp DissectionDokument5 Seiten7th Grade Shrimp DissectionWeir Kiramata100% (1)
- Disseminated Intravascular Coagulation (DIC) During Pregnancy - Clinical Findings, Etiology, and Diagnosis - UpToDateDokument23 SeitenDisseminated Intravascular Coagulation (DIC) During Pregnancy - Clinical Findings, Etiology, and Diagnosis - UpToDateCristinaCaprosNoch keine Bewertungen
- Biology Presentation Class 7Dokument11 SeitenBiology Presentation Class 7binu biju100% (2)
- Dropsy of Fetal Membran - Ther-601Dokument13 SeitenDropsy of Fetal Membran - Ther-601Bilal KhanNoch keine Bewertungen
- Digestion Science Form 2Dokument25 SeitenDigestion Science Form 2tengkusuhaidaNoch keine Bewertungen
- DP1-SL - Unit Assessment AnswersDokument12 SeitenDP1-SL - Unit Assessment AnswersAmeen amediNoch keine Bewertungen
- Levels of Biological OrganizationDokument36 SeitenLevels of Biological OrganizationClaudene GellaNoch keine Bewertungen
- Anterior Triangle of The Neck Dr. BanezDokument6 SeitenAnterior Triangle of The Neck Dr. BanezMelissa SalayogNoch keine Bewertungen
- Excretory System WorksheetDokument4 SeitenExcretory System Worksheetandresorellanab100% (2)
- PY40 - BIO - GROUP3The Somatic Nervous SystemDokument22 SeitenPY40 - BIO - GROUP3The Somatic Nervous SystemAdéọlá OnasanyaNoch keine Bewertungen
- Chapter 12 Great Vessels in The AbdomenDokument36 SeitenChapter 12 Great Vessels in The AbdomenMACON824Noch keine Bewertungen
- Tumores HepaticosDokument77 SeitenTumores HepaticosAnita Villanueva ArandaNoch keine Bewertungen
- BIO210 Lab Report 3Dokument6 SeitenBIO210 Lab Report 3Isra MallaNoch keine Bewertungen