Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Irb DocumentsDokument17 SeitenIrb Documentsapi-486275760Noch keine Bewertungen
- Understanding Self Components of Self Self Concept Self Confidence Self Image Sabnam BasuDokument28 SeitenUnderstanding Self Components of Self Self Concept Self Confidence Self Image Sabnam BasuRoldan Dela CruzNoch keine Bewertungen
- Acupressure Points ForDokument17 SeitenAcupressure Points ForAbdul Basith Shaikh100% (1)
- Biochemistry of The Eye, 2ed. 2003Dokument331 SeitenBiochemistry of The Eye, 2ed. 2003Vuqar100% (3)
- Biopsychology NotesDokument5 SeitenBiopsychology NotesPatricia100% (1)
- MM TemperamentsDokument27 SeitenMM TemperamentsKalpesh Jain100% (2)
- Jurnal MataDokument7 SeitenJurnal MatatrianaamaliaNoch keine Bewertungen
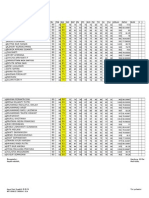
- Leger 9GDokument6 SeitenLeger 9GFaridhatulNoch keine Bewertungen
- TrobamycinDokument5 SeitenTrobamycinFaridhatulNoch keine Bewertungen
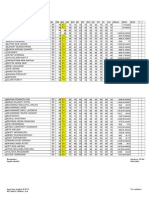
- Leger 9G Semester2Dokument6 SeitenLeger 9G Semester2FaridhatulNoch keine Bewertungen
- Anti ObesityDokument19 SeitenAnti ObesityFaridhatulNoch keine Bewertungen
- Anemia Penyakit KronikDokument12 SeitenAnemia Penyakit KronikFaridhatulNoch keine Bewertungen
- Bio Project On Immunity Class 12Dokument19 SeitenBio Project On Immunity Class 12fizakouser1216100% (1)
- Biology 211 Final Exam Study Guide 2016Dokument4 SeitenBiology 211 Final Exam Study Guide 2016GregNoch keine Bewertungen
- Digestive System Choice Board #1 Jan 2-4, 2012Dokument3 SeitenDigestive System Choice Board #1 Jan 2-4, 2012abisantiago6131Noch keine Bewertungen
- Peng2020 EFEK VITAMIN D PADA OBATDokument10 SeitenPeng2020 EFEK VITAMIN D PADA OBATrifkiNoch keine Bewertungen
- Cell Structure-WPS OfficeDokument18 SeitenCell Structure-WPS OfficeyennaNoch keine Bewertungen
- The Desmosome: Cell Science Lessons From Human Diseases: 797 CommentaryDokument10 SeitenThe Desmosome: Cell Science Lessons From Human Diseases: 797 CommentaryKatja BadanjakNoch keine Bewertungen
- Cerevisiae and Other Fungi: Principles of Gene Manipulation by Liuzengran Hebei University of Economics and BusinessDokument81 SeitenCerevisiae and Other Fungi: Principles of Gene Manipulation by Liuzengran Hebei University of Economics and BusinessManuel DíazNoch keine Bewertungen
- Should CO2 Be A Critical Process Parameter WhiteDokument4 SeitenShould CO2 Be A Critical Process Parameter WhitesalemNoch keine Bewertungen
- Histo Embryo 080622pdfDokument9 SeitenHisto Embryo 080622pdfShia LevyNoch keine Bewertungen
- Reproductive System With HighlightsDokument150 SeitenReproductive System With HighlightsReinand Joseff ServanoNoch keine Bewertungen
- Pokemon Learning League The HeartDokument26 SeitenPokemon Learning League The HeartTimothy WhitfieldNoch keine Bewertungen
- The Wishing WellDokument160 SeitenThe Wishing WellAldrin Nigel A. PascuaNoch keine Bewertungen
- 4-Blood (Hematopoiesis-Leukopoiesis) PDFDokument9 Seiten4-Blood (Hematopoiesis-Leukopoiesis) PDFUmair IkhlaqNoch keine Bewertungen
- Polygala Senega SenegaDokument4 SeitenPolygala Senega Senegaabdelaziz_ismail685662Noch keine Bewertungen
- Sarala Birla Gyan Jyoti UNIT TEST (2021-22) Subject-Science Class - XDokument5 SeitenSarala Birla Gyan Jyoti UNIT TEST (2021-22) Subject-Science Class - XsahurediffNoch keine Bewertungen
- Ayushman Spageric HerbalsDokument6 SeitenAyushman Spageric HerbalssubhalekhaNoch keine Bewertungen
- IARI PHD Entrance Question Paper 2011 - Molecular Biology and BiotechnologyDokument14 SeitenIARI PHD Entrance Question Paper 2011 - Molecular Biology and BiotechnologyAbhay Kumar100% (8)
- Feeding A Racing GreyhoundDokument11 SeitenFeeding A Racing GreyhoundsantiagobaldezNoch keine Bewertungen
- Case Study-Infant With Fluid Imbalance08-10-KEYDokument3 SeitenCase Study-Infant With Fluid Imbalance08-10-KEYreecoleNoch keine Bewertungen
- Chynna Ashley Gonzales Pendon RNDokument33 SeitenChynna Ashley Gonzales Pendon RNChynna Ashley Gonzales PendonNoch keine Bewertungen
- Chapter 10 - Respiratory System - 2020 - The Zebrafish in Biomedical ResearchDokument5 SeitenChapter 10 - Respiratory System - 2020 - The Zebrafish in Biomedical ResearchNicolas BaronNoch keine Bewertungen
- Analgesic Action of The New Drug SemaxDokument3 SeitenAnalgesic Action of The New Drug SemaxmatsapoNoch keine Bewertungen
- A Textbook of Clinical Pharmacology and Therapeutics PDFDokument6 SeitenA Textbook of Clinical Pharmacology and Therapeutics PDFMovie Box MoviesNoch keine Bewertungen
- TARIF PRODIA TAHUN 2019 Rev 2Dokument9 SeitenTARIF PRODIA TAHUN 2019 Rev 2cici100% (1)