Das könnte Ihnen auch gefallen
- Special Operations Forces Medical HandbookVon EverandSpecial Operations Forces Medical HandbookBewertung: 4.5 von 5 Sternen4.5/5 (2)
- U WORLD (Step 1) – INFECTIOUS DISEASES + MICROBIOLOGY (EDUCATIONAL OBJECTIVESDokument75 SeitenU WORLD (Step 1) – INFECTIOUS DISEASES + MICROBIOLOGY (EDUCATIONAL OBJECTIVESDrbee10Noch keine Bewertungen
- Medicine & Pediatric SMLE Notes: Key Points for ExamsDokument23 SeitenMedicine & Pediatric SMLE Notes: Key Points for Examsanmar alkhudhri100% (1)
- Pathophysiology Examination AnswersDokument205 SeitenPathophysiology Examination AnswersFırat Güllü67% (6)
- Adenotonsillitis NewDokument100 SeitenAdenotonsillitis NewDrravikumar Bhandari100% (1)
- Adult Infectious Disease Bulletpoints HandbookVon EverandAdult Infectious Disease Bulletpoints HandbookBewertung: 4.5 von 5 Sternen4.5/5 (9)
- Syphilis: Etiology, Pathogenesis, Transmission, Stages, Manifestations and TreatmentDokument39 SeitenSyphilis: Etiology, Pathogenesis, Transmission, Stages, Manifestations and TreatmentEINSTEIN2D100% (1)
- MD PPTDokument105 SeitenMD PPTtoxiczarrar.pubgNoch keine Bewertungen
- DR As TuberculosisDokument59 SeitenDR As TuberculosisAchhar SinghNoch keine Bewertungen
- Microbiology: Eukaryotes & ProkaryotesDokument7 SeitenMicrobiology: Eukaryotes & ProkaryotesJohn Christopher Luces100% (1)
- Tuberculosis PowerpointDokument69 SeitenTuberculosis PowerpointCeline Villo100% (1)
- Rash Guide Provides Descriptions of Common Childhood RashesDokument58 SeitenRash Guide Provides Descriptions of Common Childhood Rashesbashir019Noch keine Bewertungen
- Communicable Disease NursingDokument41 SeitenCommunicable Disease NursingBJ DUQUESA100% (2)
- Pharyngitis: Departemen T.H.T.K.L Fakultas Kedokteran Universitas PadjadjaranDokument64 SeitenPharyngitis: Departemen T.H.T.K.L Fakultas Kedokteran Universitas PadjadjaranEtusCelloNoch keine Bewertungen
- 2017.03.23 - Dr. Ricky Yue - LaryngitisDokument60 Seiten2017.03.23 - Dr. Ricky Yue - LaryngitisLezard DomiNoch keine Bewertungen
- Pharyngitis: Dr.M.KarimiDokument60 SeitenPharyngitis: Dr.M.KarimiJessa AdenigNoch keine Bewertungen
- Presentation URTI& LRTI - G1Dokument134 SeitenPresentation URTI& LRTI - G1Aniq Zahran MasomNoch keine Bewertungen
- San Lazaro Question Bank SouthPark 2Dokument9 SeitenSan Lazaro Question Bank SouthPark 2Kenneth MiguelNoch keine Bewertungen
- Gram (-) Cocci: NeisseriaceaeDokument8 SeitenGram (-) Cocci: NeisseriaceaeMary Grace RiveraNoch keine Bewertungen
- LimfadenitisDokument24 SeitenLimfadenitisrahmah ningsihNoch keine Bewertungen
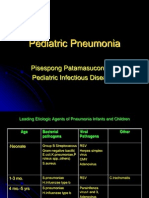
- Pediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesDokument39 SeitenPediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesSi PuputNoch keine Bewertungen
- Pharyngitis 0104 SlidesDokument144 SeitenPharyngitis 0104 SlidesZammira MutiaNoch keine Bewertungen
- L - 2 - GR (-) CocciDokument82 SeitenL - 2 - GR (-) CocciFahim NadvyNoch keine Bewertungen
- Antifungals PPTDokument29 SeitenAntifungals PPTzeenatkhatoon78Noch keine Bewertungen
- Paul Kolesnyk: Cold-Practical Approach of Family DoctorDokument34 SeitenPaul Kolesnyk: Cold-Practical Approach of Family Doctoranon_20012817Noch keine Bewertungen
- Acute Respiratory Tract InfectionDokument70 SeitenAcute Respiratory Tract InfectionCorina OngNoch keine Bewertungen
- National Antibiotic Pedia GuidelinesDokument149 SeitenNational Antibiotic Pedia GuidelinesGg GreyNoch keine Bewertungen
- Pneumonia in Children: Causes, Symptoms and TreatmentDokument27 SeitenPneumonia in Children: Causes, Symptoms and Treatmentsebghatullah mubarezNoch keine Bewertungen
- The Agent:: Mycobacterium TuberculosisDokument43 SeitenThe Agent:: Mycobacterium TuberculosisArya A MNoch keine Bewertungen
- 25.suppurative Lung DiseasesDokument6 Seiten25.suppurative Lung DiseasesDIVEN SolvonNoch keine Bewertungen
- ASOMDokument41 SeitenASOMArunkumar S KumarNoch keine Bewertungen
- Pathogens That Involve The Respiratory TractDokument28 SeitenPathogens That Involve The Respiratory TractLeeShauran100% (2)
- Tuberculosis: DR .. Magdi Elbaloola Ahmed Physcian & GastrohepatologistDokument59 SeitenTuberculosis: DR .. Magdi Elbaloola Ahmed Physcian & GastrohepatologistÅbübâkêř Äbd-ëřhēēm BãřřîNoch keine Bewertungen
- Lung Parasitic InfectionsDokument71 SeitenLung Parasitic InfectionswaheedaNoch keine Bewertungen
- Upper Respiratory Tract Infections.: DR Abdelmoniem Saeed MohammedDokument47 SeitenUpper Respiratory Tract Infections.: DR Abdelmoniem Saeed MohammedYousef Al-AmeenNoch keine Bewertungen
- I-1B. Bacterial Infection 2Dokument6 SeitenI-1B. Bacterial Infection 2Soad ShedeedNoch keine Bewertungen
- 2. Pelvic Inflammatory DiseaseDokument25 Seiten2. Pelvic Inflammatory DiseasedeepaNoch keine Bewertungen
- Respiratory Tract MicrobiologyDokument68 SeitenRespiratory Tract Microbiologysultan khabeebNoch keine Bewertungen
- Staph Infection & HIV (GP B1)Dokument48 SeitenStaph Infection & HIV (GP B1)Jared Khoo Er HauNoch keine Bewertungen
- Pharyngitis Diagnosis and TreatmentDokument27 SeitenPharyngitis Diagnosis and TreatmentSubhada GosaviNoch keine Bewertungen
- How STDs SpreadDokument55 SeitenHow STDs Spreadjoshy221196Noch keine Bewertungen
- Journal Reading: Management of Acute Suppurative ParotitisDokument13 SeitenJournal Reading: Management of Acute Suppurative ParotitisNoritaAprilyaSiswandeviNoch keine Bewertungen
- Diphtheria HandoutsDokument8 SeitenDiphtheria HandoutsRachelle Mae DimayugaNoch keine Bewertungen
- Municable DiseasesDokument18 SeitenMunicable DiseasesEdamarie ChuaNoch keine Bewertungen
- Diagnosis of Oral InfectionDokument72 SeitenDiagnosis of Oral InfectionMohit_Gupta_9876Noch keine Bewertungen
- Febrile Neutropenia ArunDokument40 SeitenFebrile Neutropenia ArunArun GeorgeNoch keine Bewertungen
- Infectious DiseasesDokument140 SeitenInfectious DiseasesSamah IzzNoch keine Bewertungen
- Understanding Chlamydiae InfectionsDokument32 SeitenUnderstanding Chlamydiae InfectionsNaing Lin SoeNoch keine Bewertungen
- Bacterial Infection On Respiration Tract: Ike Irmawati P.A, Msi Med Mikrobiologi FK YarsiDokument39 SeitenBacterial Infection On Respiration Tract: Ike Irmawati P.A, Msi Med Mikrobiologi FK YarsiCamila SuhendarNoch keine Bewertungen
- Scrub Typhus: Causes, Symptoms and TreatmentDokument35 SeitenScrub Typhus: Causes, Symptoms and TreatmentdrgaviNoch keine Bewertungen
- Omphalitis LectureDokument18 SeitenOmphalitis LectureWonyenghitari George0% (1)
- PNEUMONIADokument44 SeitenPNEUMONIAReshama JamankarNoch keine Bewertungen
- Presenter: clerk 2 蘇雋淋 Date: 2022/03/11Dokument39 SeitenPresenter: clerk 2 蘇雋淋 Date: 2022/03/11s0501120醫學系Noch keine Bewertungen
- Abx De-Escalation OutlineDokument6 SeitenAbx De-Escalation Outlineapi-648401824Noch keine Bewertungen
- MTS - Fever and Chills in ChildrenDokument36 SeitenMTS - Fever and Chills in ChildrenYayaNoch keine Bewertungen
- CNS Infections 2013 - MKDokument54 SeitenCNS Infections 2013 - MKmicroperadeniyaNoch keine Bewertungen
- Recurrent Respiratory Papillomatosis: FaringDokument49 SeitenRecurrent Respiratory Papillomatosis: FaringIchsanJuliansyahNoch keine Bewertungen
- Oxygen Saturation (If Available) : IagnosisDokument3 SeitenOxygen Saturation (If Available) : Iagnosisrezairfan221Noch keine Bewertungen
- Pulmonar y TuberculosisDokument35 SeitenPulmonar y TuberculosistuyalimonNoch keine Bewertungen
- สำเนา pharyngitisDokument47 Seitenสำเนา pharyngitisThanawat SimaNoch keine Bewertungen
- Communicable DiseasesDokument162 SeitenCommunicable DiseasesCarlo VigoNoch keine Bewertungen
- SketchyDokument3 SeitenSketchybellNoch keine Bewertungen
- Guide to Pediatric Urology and Surgery in Clinical PracticeVon EverandGuide to Pediatric Urology and Surgery in Clinical PracticeNoch keine Bewertungen
- HematologyDokument37 SeitenHematologykurt Allen MacarilayNoch keine Bewertungen
- Antirheumatic and Antigout DrugsDokument66 SeitenAntirheumatic and Antigout DrugsBadri KarkiNoch keine Bewertungen
- Ken's Thesis Chapter 1-6 Main WK Final Final For PrintDokument56 SeitenKen's Thesis Chapter 1-6 Main WK Final Final For PrintCallumNoch keine Bewertungen
- Test Result Normal Range Interpreta Tion Implicatio NDokument11 SeitenTest Result Normal Range Interpreta Tion Implicatio NSitty Aizah MangotaraNoch keine Bewertungen
- Management Syok Anafilaktik UnbrahDokument31 SeitenManagement Syok Anafilaktik UnbrahSasha ManoNoch keine Bewertungen
- Reducing Malaria Infections in Sub-Saharan AfricaDokument2 SeitenReducing Malaria Infections in Sub-Saharan AfricaStansa SeniaNoch keine Bewertungen
- Yanzen Bagus Setiawan: Name: Date of Birth: Sex: NationalityDokument1 SeiteYanzen Bagus Setiawan: Name: Date of Birth: Sex: NationalitylisaNoch keine Bewertungen
- CHAPTER 5 InflammationDokument51 SeitenCHAPTER 5 Inflammationyeshita yonasNoch keine Bewertungen
- 2014 Bauman - 4th Chapter 14Dokument20 Seiten2014 Bauman - 4th Chapter 14add100% (1)
- Leflet Asmpid New-3Dokument1 SeiteLeflet Asmpid New-3TheAru21Noch keine Bewertungen
- West Nile FeverDokument23 SeitenWest Nile Fevertummalapalli venkateswara raoNoch keine Bewertungen
- Herpes Zoster in Diverse Situations - A Review PDFDokument21 SeitenHerpes Zoster in Diverse Situations - A Review PDFLaras KinasihNoch keine Bewertungen
- Origin, Transmission, Diagnosis and Management of Coronavirus Disease 2019 (COVID-19)Dokument6 SeitenOrigin, Transmission, Diagnosis and Management of Coronavirus Disease 2019 (COVID-19)Alfitrah NurjayaNoch keine Bewertungen
- Acute GastroenteritisDokument48 SeitenAcute Gastroenteritisansam kamalNoch keine Bewertungen
- MeningitisDokument12 SeitenMeningitisFaith Vaughn100% (2)
- Necrotizing Fasciitis (Autosaved)Dokument23 SeitenNecrotizing Fasciitis (Autosaved)19-1 NUR ALIMNoch keine Bewertungen
- Referat Malaria InovDokument29 SeitenReferat Malaria InovAssifa RidzkiNoch keine Bewertungen
- Approach To The Patient With Facial Erythema PDFDokument38 SeitenApproach To The Patient With Facial Erythema PDFFilipa FigueiredoNoch keine Bewertungen
- Blood Cell Formation (Hematopoiesis) : Senin, 12 Januari 2004Dokument42 SeitenBlood Cell Formation (Hematopoiesis) : Senin, 12 Januari 2004nurliah armandNoch keine Bewertungen
- Cicrulatory and Immune Workbook KEYDokument32 SeitenCicrulatory and Immune Workbook KEYgeorgia robinsonNoch keine Bewertungen
- BronchioitisDokument24 SeitenBronchioitismitiku aberaNoch keine Bewertungen
- Opportunistic Mycoses: Portal of Entry: Respiratory, Mucocutaneous Infectious Particles: Conidia, MyceliaDokument4 SeitenOpportunistic Mycoses: Portal of Entry: Respiratory, Mucocutaneous Infectious Particles: Conidia, MyceliaPinay YaunNoch keine Bewertungen
- Science As Human Endeavour TaskDokument2 SeitenScience As Human Endeavour Taskyolanda Sitepu100% (1)
- Arbovirus EpidemiologyDokument48 SeitenArbovirus EpidemiologyEdward ChavezNoch keine Bewertungen
- Medical Entrance Form (Required) : Georgia Institute of Technology Please Fax Your Completed Form To 404-385-0329Dokument4 SeitenMedical Entrance Form (Required) : Georgia Institute of Technology Please Fax Your Completed Form To 404-385-0329Elizabeth ZaldivarNoch keine Bewertungen
- Hubungan Pengetahuan Terhadap Perilaku Penggunaan Suplemen Kesehatan Warga Kebonsari Surabaya Di Masa Pandemi Covid-19Dokument6 SeitenHubungan Pengetahuan Terhadap Perilaku Penggunaan Suplemen Kesehatan Warga Kebonsari Surabaya Di Masa Pandemi Covid-19SavaNoch keine Bewertungen
- 2022PET JZ FIA VETCHECK Brochures Ver - JZDokument12 Seiten2022PET JZ FIA VETCHECK Brochures Ver - JZAsesoria TecnicaNoch keine Bewertungen