Das könnte Ihnen auch gefallen
- Skin Cancer ShowDokument57 SeitenSkin Cancer ShowNice YouNoch keine Bewertungen
- (Mebooksfree Net) Hin&atl&uro&sur&4thDokument967 Seiten(Mebooksfree Net) Hin&atl&uro&sur&4thMohammadSAL-Rawashdeh100% (12)
- Squamous Cell Carcinoma-Well DifferentiatedDokument4 SeitenSquamous Cell Carcinoma-Well DifferentiatedYukankolmi OyoNoch keine Bewertungen
- (Mebooksfree Net) Pri&pra&uro&sal&2&vol&set&2ndDokument1.235 Seiten(Mebooksfree Net) Pri&pra&uro&sal&2&vol&set&2ndMohammadSAL-Rawashdeh100% (1)
- Lymph Nodes of Head and Neck RegionDokument65 SeitenLymph Nodes of Head and Neck RegionpreyasjoshiNoch keine Bewertungen
- Causes and Treatment of Malignant Melanoma: DiscussionDokument4 SeitenCauses and Treatment of Malignant Melanoma: DiscussionAriSeliengNoch keine Bewertungen
- Dr. C.T. Karthikeyan, Associate Professor, Dept. of General SurgeryDokument40 SeitenDr. C.T. Karthikeyan, Associate Professor, Dept. of General SurgeryNaveen RajeshwarNoch keine Bewertungen
- Liver Cancer Pathophysiology: Predisposing FactorDokument3 SeitenLiver Cancer Pathophysiology: Predisposing FactorTarantado100% (2)
- Cancer of The PenisDokument6 SeitenCancer of The PenisPaul CenabreNoch keine Bewertungen
- (Mebooksfree Net) Oxf&tex&uro&sur&1stDokument1.201 Seiten(Mebooksfree Net) Oxf&tex&uro&sur&1stMohammadSAL-Rawashdeh100% (2)
- Basal Cell Carcinoma - Pathophysiology and ManagementDokument6 SeitenBasal Cell Carcinoma - Pathophysiology and ManagementReylan Garcia0% (1)
- Nursing Care Management 106Dokument82 SeitenNursing Care Management 106maynard baird100% (6)
- The Breast - Comprehensive Management of Benign and Malignant Diseases 5e WWW Bookbaz IrDokument1.435 SeitenThe Breast - Comprehensive Management of Benign and Malignant Diseases 5e WWW Bookbaz Irzahra mNoch keine Bewertungen
- Specialty Certificate in Medical Oncology Sample QuestionsDokument27 SeitenSpecialty Certificate in Medical Oncology Sample Questionsvimal raj100% (1)
- Practical Management of Thyroid Cancer A Multidisciplinary Approach 2nd EditionDokument386 SeitenPractical Management of Thyroid Cancer A Multidisciplinary Approach 2nd EditionAd Adriana100% (1)
- Skin Cancers. Malignant MelanomaDokument53 SeitenSkin Cancers. Malignant MelanomaАбдул Насер МохаммадізмаелNoch keine Bewertungen
- PATHOLOGYDokument188 SeitenPATHOLOGYMaisha Maliha ShamsNoch keine Bewertungen
- Bab TerakirDokument86 SeitenBab TerakirDian Asri Gumilang PratiwiNoch keine Bewertungen
- Skin CancerDokument7 SeitenSkin Cancerعبدالعزيز احمد علي عتشNoch keine Bewertungen
- Melanoma: Meku Damtie (M.D.) July 18, 2006Dokument38 SeitenMelanoma: Meku Damtie (M.D.) July 18, 2006Worku KifleNoch keine Bewertungen
- Skin CancerDokument5 SeitenSkin CancerEl FaroukNoch keine Bewertungen
- Diagnosis and Treatment of MelanomaDokument14 SeitenDiagnosis and Treatment of MelanomaAnonymous Af24L7Noch keine Bewertungen
- Subcutaneous MetsDokument27 SeitenSubcutaneous MetsDavidJohnsonNoch keine Bewertungen
- Malignant Epithelial NeoplasmsDokument19 SeitenMalignant Epithelial NeoplasmsAtef Mahmoud AhmedNoch keine Bewertungen
- 2008-Malignant Epidermal TumorsDokument58 Seiten2008-Malignant Epidermal Tumorsapi-19916399Noch keine Bewertungen
- SKIN CANCER by Shahid and Nawaira PthologyDokument31 SeitenSKIN CANCER by Shahid and Nawaira PthologyShahid BashirNoch keine Bewertungen
- PathologyDokument58 SeitenPathologysankethg93Noch keine Bewertungen
- Beware of MelanomaDokument5 SeitenBeware of MelanomaBala SubramanianNoch keine Bewertungen
- Metastatic Malignant Melanoma: A Case StudyDokument3 SeitenMetastatic Malignant Melanoma: A Case StudyDyerik LilingNoch keine Bewertungen
- Journal ReadingDokument41 SeitenJournal ReadingEndorfin AdrenalinNoch keine Bewertungen
- Maligna MelanomaDokument80 SeitenMaligna MelanomaNoveldy PitnaNoch keine Bewertungen
- Skin Cancers: Assistant Larisa PoroshinaDokument42 SeitenSkin Cancers: Assistant Larisa PoroshinaMed PoxNoch keine Bewertungen
- Malignant Epithelial Non-Odontogenic Tumors 2Dokument11 SeitenMalignant Epithelial Non-Odontogenic Tumors 2samamustafa.2003Noch keine Bewertungen
- Garbe2007 PDFDokument7 SeitenGarbe2007 PDFArsen NitNoch keine Bewertungen
- MelanomaDokument11 SeitenMelanomaAriSeliengNoch keine Bewertungen
- Skin Lesion DiagnosisDokument9 SeitenSkin Lesion DiagnosisaequNoch keine Bewertungen
- Managing Malignant Melanoma: Learning Objectives: After Reading This Article, The Participant Should Be AbleDokument15 SeitenManaging Malignant Melanoma: Learning Objectives: After Reading This Article, The Participant Should Be AbleDian Ariska SNoch keine Bewertungen
- Skin Cancer TBL 2 2f3Dokument19 SeitenSkin Cancer TBL 2 2f3api-356476029Noch keine Bewertungen
- Presentation 3Dokument14 SeitenPresentation 3Linda Lam100% (1)
- ONCOLOGICAL GYNECOLOGY-Malignant Diseases of The Vulva and Modalities of Treatment by Prof - Dr.Vesna AntovskaDokument22 SeitenONCOLOGICAL GYNECOLOGY-Malignant Diseases of The Vulva and Modalities of Treatment by Prof - Dr.Vesna AntovskaVesna AntovskaNoch keine Bewertungen
- Basic Plastic + Skin CancerDokument29 SeitenBasic Plastic + Skin CancermitaNoch keine Bewertungen
- Mrs. Maria Susan Z. MaglaquiDokument5 SeitenMrs. Maria Susan Z. MaglaquiRon Agustin JrNoch keine Bewertungen
- Melanoma Belay Z July, 6 2005Dokument20 SeitenMelanoma Belay Z July, 6 2005Worku KifleNoch keine Bewertungen
- Surgical Treatment of Melanoma: Acta Chirurgiae Plasticae April 2018Dokument8 SeitenSurgical Treatment of Melanoma: Acta Chirurgiae Plasticae April 2018alexandru_andreaNoch keine Bewertungen
- AnaPhy Skin Cancer Case Study-BASCODokument6 SeitenAnaPhy Skin Cancer Case Study-BASCOChristine Jane BascoNoch keine Bewertungen
- Skin Cancer FinalDokument9 SeitenSkin Cancer Finalapi-609308130Noch keine Bewertungen
- Midgut Volvulus ABSTRACTDokument27 SeitenMidgut Volvulus ABSTRACTely saktiNoch keine Bewertungen
- Anal Melanoma: Marc Singer, M.D. and Matthew G. Mutch, M.DDokument10 SeitenAnal Melanoma: Marc Singer, M.D. and Matthew G. Mutch, M.DbkiriazovNoch keine Bewertungen
- Nodular Malignant Melanoma: Case ReportDokument13 SeitenNodular Malignant Melanoma: Case ReportasclepiuspdfsNoch keine Bewertungen
- Skin Cancer Лекция - 2 Дополненная Перевод - КопияDokument72 SeitenSkin Cancer Лекция - 2 Дополненная Перевод - Копияdrmedico82Noch keine Bewertungen
- Nonsquamous Cell Malignant Tumours of The Oral Cavity: An OverviewDokument6 SeitenNonsquamous Cell Malignant Tumours of The Oral Cavity: An OverviewranggadrNoch keine Bewertungen
- English Assignment: Ni Made Desi Sugiani P07120214017Dokument10 SeitenEnglish Assignment: Ni Made Desi Sugiani P07120214017Tia Nagzz WbsNoch keine Bewertungen
- Malignant Melanoma Research PaperDokument10 SeitenMalignant Melanoma Research Paperapi-272931142Noch keine Bewertungen
- Squamous Cell Skin CancerDokument2 SeitenSquamous Cell Skin CancerToni Mas IrwandaNoch keine Bewertungen
- Djohan2010bening&malignan TumorDokument13 SeitenDjohan2010bening&malignan TumorkikiNoch keine Bewertungen
- Conjunctival Pigmented LesionsDokument0 SeitenConjunctival Pigmented LesionsBhartendu Agarwal0% (1)
- MelanomaDokument32 SeitenMelanomaAishwaryaNoch keine Bewertungen
- Malignant Tumors: Dr.N.Govindrajkumar Reader Dept - Oral &maxillo Facial PathologyDokument50 SeitenMalignant Tumors: Dr.N.Govindrajkumar Reader Dept - Oral &maxillo Facial PathologypriyaNoch keine Bewertungen
- Skin Tumors: Dr. Ihsan Al-Turfy Consultant Dermatologist College of Medicine/Baghdad MBCHB, DDV, Ficms, CabdDokument149 SeitenSkin Tumors: Dr. Ihsan Al-Turfy Consultant Dermatologist College of Medicine/Baghdad MBCHB, DDV, Ficms, CabdRomi WijiantoNoch keine Bewertungen
- Skin LesionDokument23 SeitenSkin Lesion5alifa55Noch keine Bewertungen
- وسام عوض Benign Skin Tumor-5 (Muhadharaty)Dokument6 Seitenوسام عوض Benign Skin Tumor-5 (Muhadharaty)Alaa AhmedNoch keine Bewertungen
- Squamous Cell CarcinomaDokument3 SeitenSquamous Cell CarcinomaJohn HanNaNoch keine Bewertungen
- Akin CancerDokument7 SeitenAkin Cancerucul8Noch keine Bewertungen
- Presentation 1Dokument31 SeitenPresentation 1Nice YouNoch keine Bewertungen
- Current Controversies in The Management of Malignant Parotid TumorsDokument8 SeitenCurrent Controversies in The Management of Malignant Parotid TumorsDirga Rasyidin LNoch keine Bewertungen
- Sheet 11 PDFDokument16 SeitenSheet 11 PDFHanin AbukhiaraNoch keine Bewertungen
- Tumors of External and Middle EarDokument42 SeitenTumors of External and Middle EarAmiteshwar SinghNoch keine Bewertungen
- Atlas of Diagnostically Challenging Melanocytic NeoplasmsVon EverandAtlas of Diagnostically Challenging Melanocytic NeoplasmsNoch keine Bewertungen
- Sylfonylurea: Class Generic Trade Store NotesDokument4 SeitenSylfonylurea: Class Generic Trade Store NotesMohammadSAL-RawashdehNoch keine Bewertungen
- Chapter #55 - Physiology and Pharmacology of The Renal Pelvis and UreterDokument6 SeitenChapter #55 - Physiology and Pharmacology of The Renal Pelvis and UreterMohammadSAL-RawashdehNoch keine Bewertungen
- 2017 Residancy Exam JUHDokument8 Seiten2017 Residancy Exam JUHMohammadSAL-RawashdehNoch keine Bewertungen
- ملخص عن حب الشبابDokument10 Seitenملخص عن حب الشبابMohammadSAL-RawashdehNoch keine Bewertungen
- كتاب اسئلة جميلDokument401 Seitenكتاب اسئلة جميلMohammadSAL-Rawashdeh100% (1)
- كتاب اسئلة جميلDokument401 Seitenكتاب اسئلة جميلMohammadSAL-Rawashdeh100% (1)
- Urology Sample MCQ Exam eDokument5 SeitenUrology Sample MCQ Exam eMohammadSAL-RawashdehNoch keine Bewertungen
- Head & Neck Cancers: Prof. Igor Y. Galaychuk, MDDokument43 SeitenHead & Neck Cancers: Prof. Igor Y. Galaychuk, MDMohammadSAL-RawashdehNoch keine Bewertungen
- Sabers HandbookDokument35 SeitenSabers HandbookMohammadSAL-Rawashdeh100% (1)
- Atlas 4 دائرة معارف طبية Reduced PDFDokument316 SeitenAtlas 4 دائرة معارف طبية Reduced PDFMohammadSAL-RawashdehNoch keine Bewertungen
- 6 - 7 - 8 Peritoneum, Pancreas, AppendixDokument134 Seiten6 - 7 - 8 Peritoneum, Pancreas, AppendixMohammadSAL-RawashdehNoch keine Bewertungen
- Oral Cancer: Oral Cancer Is A Subtype of Head and Neck Cancer, Is Any Cancerous Tissue Growth Located in The Oral CavityDokument38 SeitenOral Cancer: Oral Cancer Is A Subtype of Head and Neck Cancer, Is Any Cancerous Tissue Growth Located in The Oral CavityMohammadSAL-RawashdehNoch keine Bewertungen
- Human Immunodeficiency Virus (HIV) : Mohammad Al-Rawashdeh 54-5th CourseDokument39 SeitenHuman Immunodeficiency Virus (HIV) : Mohammad Al-Rawashdeh 54-5th CourseMohammadSAL-RawashdehNoch keine Bewertungen
- Clinicopathological Staging For Colorectal CancerDokument20 SeitenClinicopathological Staging For Colorectal Cancertr0xanNoch keine Bewertungen
- Morning Report: Pulmonology and Respiratory Medicine Medical Faculty of Sebelas Maret University 2021Dokument30 SeitenMorning Report: Pulmonology and Respiratory Medicine Medical Faculty of Sebelas Maret University 2021debby nirmasariNoch keine Bewertungen
- Chapter 9Dokument62 SeitenChapter 9Francisco GaniNoch keine Bewertungen
- Retrobulbar Tumors in Indonesia: OrbitDokument9 SeitenRetrobulbar Tumors in Indonesia: OrbitsoehartyNoch keine Bewertungen
- Seamless Care - DR SH LeungDokument38 SeitenSeamless Care - DR SH Leungmalaysianhospicecouncil6240Noch keine Bewertungen
- Spirituality, Hope and Wisdom in Cancer PatientsDokument5 SeitenSpirituality, Hope and Wisdom in Cancer PatientsIJAR JOURNALNoch keine Bewertungen
- Mechanism of Lymph Node Metastasis in Prostate CancerDokument20 SeitenMechanism of Lymph Node Metastasis in Prostate CancerAlexBritoNoch keine Bewertungen
- Evaluation of The Physicochemical Properties and Stability of SLNDokument276 SeitenEvaluation of The Physicochemical Properties and Stability of SLNvkguptajssNoch keine Bewertungen
- Cancer en Cavidad OralDokument17 SeitenCancer en Cavidad OralRafa LopezNoch keine Bewertungen
- MBC Maxwell Release 9-19-12Dokument2 SeitenMBC Maxwell Release 9-19-12Sorin IordacheNoch keine Bewertungen
- NeuroblastomaDokument9 SeitenNeuroblastomasamantha mccoyNoch keine Bewertungen
- Nhóm 6 - Fucoidan and Treatment CancerDokument18 SeitenNhóm 6 - Fucoidan and Treatment CancerThị ThiênNoch keine Bewertungen
- Tumor: Essential Neurosurgery For Medical StudentsDokument34 SeitenTumor: Essential Neurosurgery For Medical StudentsLuis PNoch keine Bewertungen
- Review of Histological Grading SystemsDokument20 SeitenReview of Histological Grading SystemsEzequiel Davi Dos SantosNoch keine Bewertungen
- Small Renal MassDokument26 SeitenSmall Renal MassSausan RasmiyyahNoch keine Bewertungen
- Oncology Case StudyDokument8 SeitenOncology Case Studyapi-273522923Noch keine Bewertungen
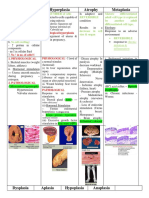
- Hypertrophy Hyperplasia Atrophy MetaplasiaDokument20 SeitenHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNoch keine Bewertungen
- Bibliograhy-Tanishka MistryDokument23 SeitenBibliograhy-Tanishka Mistryapi-512047026Noch keine Bewertungen
- 28Dokument16 Seiten28Gus RamaNoch keine Bewertungen
- Circulating Tumor Cells in Breast Cancer Metastatic DiseaseDokument177 SeitenCirculating Tumor Cells in Breast Cancer Metastatic DiseaseAd AdrianaNoch keine Bewertungen
- Irfan's Shukar BookDokument56 SeitenIrfan's Shukar BookHina MalikNoch keine Bewertungen
- Paper 8699Dokument13 SeitenPaper 8699IJARSCT JournalNoch keine Bewertungen
- Leiomyosarcoma of The BoneDokument5 SeitenLeiomyosarcoma of The BonedrjorgewtorresNoch keine Bewertungen
- Problems in Diagnosis Approach For Carcinoma of Pancreatic HeadDokument6 SeitenProblems in Diagnosis Approach For Carcinoma of Pancreatic HeadfikriafisNoch keine Bewertungen