Das könnte Ihnen auch gefallen
- Tugas RefaratDokument3 SeitenTugas RefaratBertin MallisaNoch keine Bewertungen
- Daftar PustakaDokument1 SeiteDaftar PustakaBertin MallisaNoch keine Bewertungen
- Daftar PustakaDokument1 SeiteDaftar PustakaBertin MallisaNoch keine Bewertungen
- Daftar Pustaka: Presentations and Molecular Pathology, Medknow Publications, Accessed inDokument1 SeiteDaftar Pustaka: Presentations and Molecular Pathology, Medknow Publications, Accessed inBertin MallisaNoch keine Bewertungen
- Clinical FeaturesDokument6 SeitenClinical FeaturesBertin MallisaNoch keine Bewertungen
- NIH Public Access: Author ManuscriptDokument17 SeitenNIH Public Access: Author ManuscriptBertin MallisaNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Glgq1g10 Sci Las Set 4 ColoredDokument4 SeitenGlgq1g10 Sci Las Set 4 ColoredPogi AkoNoch keine Bewertungen
- Shreya Keshari PDFDokument75 SeitenShreya Keshari PDFANKIT SINGHNoch keine Bewertungen
- PSYCHODYNAMICS AND JUDAISM The Jewish in Uences in Psychoanalysis and Psychodynamic TheoriesDokument33 SeitenPSYCHODYNAMICS AND JUDAISM The Jewish in Uences in Psychoanalysis and Psychodynamic TheoriesCarla MissionaNoch keine Bewertungen
- Letters of ComplaintDokument3 SeitenLetters of ComplaintMercedes Jimenez RomanNoch keine Bewertungen
- Birnbaum - 2006 Registration SummaryDokument14 SeitenBirnbaum - 2006 Registration SummaryEnvironmental Evaluators Network100% (1)
- Program PlanningDokument24 SeitenProgram Planningkylexian1Noch keine Bewertungen
- Oniom PDFDokument119 SeitenOniom PDFIsaac Huidobro MeezsNoch keine Bewertungen
- Walmart Assignment1Dokument13 SeitenWalmart Assignment1kingkammyNoch keine Bewertungen
- Mock Exam 2Dokument18 SeitenMock Exam 2Anna StacyNoch keine Bewertungen
- Mission Veng 29th, 2019Dokument4 SeitenMission Veng 29th, 2019Lasky ChhakchhuakNoch keine Bewertungen
- 145class 7 Integers CH 1Dokument2 Seiten145class 7 Integers CH 17A04Aditya MayankNoch keine Bewertungen
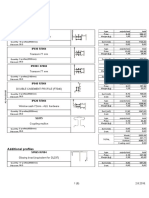
- Lista Materijala WordDokument8 SeitenLista Materijala WordAdis MacanovicNoch keine Bewertungen
- Neuralink DocumentationDokument25 SeitenNeuralink DocumentationVAIDIK Kasoju100% (6)
- Grammar Exercises AnswersDokument81 SeitenGrammar Exercises Answerspole star107100% (1)
- FUNCTIONS of LANGUAGE L. HébertDokument7 SeitenFUNCTIONS of LANGUAGE L. HébertGonzalo Muniz100% (2)
- Hermeneutical Phenomenology and Human Enviroment SystemDokument12 SeitenHermeneutical Phenomenology and Human Enviroment SystemAllen Rose Buenaflor BuenoNoch keine Bewertungen
- Government of Kerala: Minority CertificateDokument1 SeiteGovernment of Kerala: Minority CertificateBI185824125 Personal AccountingNoch keine Bewertungen
- Cayman Islands National Youth Policy September 2000Dokument111 SeitenCayman Islands National Youth Policy September 2000Kyler GreenwayNoch keine Bewertungen
- Rizal Course ReviewerDokument6 SeitenRizal Course ReviewerMarianne AtienzaNoch keine Bewertungen
- GrandEsta - Double Eyelid Surgery PDFDokument2 SeitenGrandEsta - Double Eyelid Surgery PDFaniyaNoch keine Bewertungen
- Jack Pumpkinhead of Oz - L. Frank BaumDokument68 SeitenJack Pumpkinhead of Oz - L. Frank BaumbobbyejayneNoch keine Bewertungen
- Worcester Vs Ocampo - DigestDokument1 SeiteWorcester Vs Ocampo - DigestMaria Raisa Helga YsaacNoch keine Bewertungen
- Module 7 - Prob D-E Valuation and Concepts AnswersDokument3 SeitenModule 7 - Prob D-E Valuation and Concepts Answersvenice cambryNoch keine Bewertungen
- IJONE Jan-March 2017-3 PDFDokument140 SeitenIJONE Jan-March 2017-3 PDFmoahammad bilal AkramNoch keine Bewertungen
- ERP Test BankDokument29 SeitenERP Test BankAsma 12Noch keine Bewertungen
- Wardancer 4e HomebrewDokument3 SeitenWardancer 4e HomebrewWyjecNoch keine Bewertungen
- DLL Ict 9 1st Quarter Week 5Dokument3 SeitenDLL Ict 9 1st Quarter Week 5Bernadeth Irma Sawal Caballa100% (2)
- Indonesian High School Student Motivational Orientations For Learning English As A Foreign LanguageDokument18 SeitenIndonesian High School Student Motivational Orientations For Learning English As A Foreign LanguageAlberth DalopeNoch keine Bewertungen
- The Court of Heaven 1Dokument2 SeitenThe Court of Heaven 1Rhoda Collins100% (7)
- Associate-Shopping in Hyderabad, Telangana Careers at HyderabadDokument1 SeiteAssociate-Shopping in Hyderabad, Telangana Careers at HyderabadpavanNoch keine Bewertungen