Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- RTR 160 PDFDokument74 SeitenRTR 160 PDFLukesh Kumar100% (2)
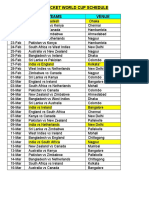
- 2011 Cricket World Cup ScheduleDokument2 Seiten2011 Cricket World Cup ScheduleVishnu RamNoch keine Bewertungen
- F1 Track Design and Safety - PPTDokument17 SeitenF1 Track Design and Safety - PPTyogesh kumarNoch keine Bewertungen
- Current Affairs November 2016 Quiz PDFDokument62 SeitenCurrent Affairs November 2016 Quiz PDFAritraRionKunduNoch keine Bewertungen
- JSA For Removal of Broken Bolts and Installation of Switch Pannel On Compressor at Process AraeDokument4 SeitenJSA For Removal of Broken Bolts and Installation of Switch Pannel On Compressor at Process AraeMohammed MinhajNoch keine Bewertungen
- KONERDokument100 SeitenKONERLenin InlagoNoch keine Bewertungen
- Paperback Adventures RulebookDokument24 SeitenPaperback Adventures RulebookEric OverkampNoch keine Bewertungen
- Senarai Ikut Bas - 05.10PMDokument2 SeitenSenarai Ikut Bas - 05.10PMDonat CoklatNoch keine Bewertungen
- Gilles VilleneuveDokument10 SeitenGilles VilleneuveWILLIAM HASSETTNoch keine Bewertungen
- Cricket PPT NewDokument31 SeitenCricket PPT NewMajid HabibNoch keine Bewertungen
- Peripheral Vascular AssessmentDokument14 SeitenPeripheral Vascular AssessmentgireeshsachinNoch keine Bewertungen
- Spider-Man 3 The Ultimate Game (2007) - RulesDokument5 SeitenSpider-Man 3 The Ultimate Game (2007) - RulesA GNoch keine Bewertungen
- Bet Slip 10Dokument4 SeitenBet Slip 10Jordi NaibahoNoch keine Bewertungen
- Race To Tokyo - BWF Olympic Qualification - 18-05-2021 - .XLSX MSDokument2 SeitenRace To Tokyo - BWF Olympic Qualification - 18-05-2021 - .XLSX MSAngga KusumanataNoch keine Bewertungen
- Apollo and DaphneDokument2 SeitenApollo and DaphneYftisham L MangrayNoch keine Bewertungen
- Svoronos J.N. Ta Nomismata Tou Kratous Ton Ptolemaion (Ptolemaic Coinage) - 1904Dokument397 SeitenSvoronos J.N. Ta Nomismata Tou Kratous Ton Ptolemaion (Ptolemaic Coinage) - 1904CassivelanNoch keine Bewertungen
- Pages From 05-01269 Regeneration API-617-datasheet-rev11 PDFDokument1 SeitePages From 05-01269 Regeneration API-617-datasheet-rev11 PDFalikajbafNoch keine Bewertungen
- Bosch SDL 260 ManualDokument3 SeitenBosch SDL 260 ManualMarian AdrianNoch keine Bewertungen
- YALE (A955) ERP16VF EUROPE FORKLIFT Service Repair Manual PDFDokument17 SeitenYALE (A955) ERP16VF EUROPE FORKLIFT Service Repair Manual PDFfhjskemmd50% (2)
- Say My NameDokument4 SeitenSay My NameAnne LunaNoch keine Bewertungen
- Resultof1stEntryTest 2019 23-6-2019Dokument298 SeitenResultof1stEntryTest 2019 23-6-2019muhammadNoch keine Bewertungen
- 2GMYDokument100 Seiten2GMYalcowoNoch keine Bewertungen
- README!Dokument2 SeitenREADME!Ronakdeep BhatiaNoch keine Bewertungen
- Up 180 15762Dokument2.303 SeitenUp 180 15762Uday kumarNoch keine Bewertungen
- The Duggins-Briggs Fortune Telling Card MeaningsDokument1 SeiteThe Duggins-Briggs Fortune Telling Card Meaningssunoflight396100% (3)
- Fighter - Tactician Martial Archetype (8933850)Dokument3 SeitenFighter - Tactician Martial Archetype (8933850)Heath WannemacherNoch keine Bewertungen
- Iron Game HistoryDokument12 SeitenIron Game Historysteppenwolf88100% (1)
- Manual - Usuario - Air Rower Machine User Manual (WJ-8043)Dokument10 SeitenManual - Usuario - Air Rower Machine User Manual (WJ-8043)CosmeNoch keine Bewertungen
- Ryobi: 18 Volt Circular Saw Model No. P508 Repair SheetDokument4 SeitenRyobi: 18 Volt Circular Saw Model No. P508 Repair SheetVictor Perez100% (1)
- Callan Kids Level1bDokument10 SeitenCallan Kids Level1bThanh TranNoch keine Bewertungen