Das könnte Ihnen auch gefallen
- Emirates International University Faculty of Pharmacy Pharmacoeconomic Lecno3Dokument27 SeitenEmirates International University Faculty of Pharmacy Pharmacoeconomic Lecno3علي الطياريNoch keine Bewertungen
- Pe 1Dokument36 SeitenPe 1zahraaajeel993Noch keine Bewertungen
- Evidence Based Medicine: Health EconomicsDokument23 SeitenEvidence Based Medicine: Health EconomicsdrgrizahNoch keine Bewertungen
- Comprehensive Pharmacy Review For NAPLEX 8th Ed - Chapter 54Dokument50 SeitenComprehensive Pharmacy Review For NAPLEX 8th Ed - Chapter 54DrSamia El WakilNoch keine Bewertungen
- MUCLecture 2022 81832586Dokument10 SeitenMUCLecture 2022 81832586hospitalpharmacist23Noch keine Bewertungen
- Pharmacoeconomics - : Lebanese International University School of Pharmacy Fall 2021-2022Dokument50 SeitenPharmacoeconomics - : Lebanese International University School of Pharmacy Fall 2021-2022undeadrebornNoch keine Bewertungen
- Pharmacoeconomics - Part IDokument28 SeitenPharmacoeconomics - Part ISima JabbariNoch keine Bewertungen
- Perspectives in Pharmacoeconomic Evaluation L3 Part 1Dokument16 SeitenPerspectives in Pharmacoeconomic Evaluation L3 Part 1aleen qawareetNoch keine Bewertungen
- Prepared By: ASMA M A First M.Pharm PharmacologyDokument25 SeitenPrepared By: ASMA M A First M.Pharm Pharmacologyhumag143100% (1)
- Hospital PricingDokument41 SeitenHospital Pricingaarti HingeNoch keine Bewertungen
- Pharmacoeconomics 3rd Prof.Dokument64 SeitenPharmacoeconomics 3rd Prof.Ahmed ImranNoch keine Bewertungen
- Pharmacoeconomics CompiledDokument53 SeitenPharmacoeconomics CompiledMuhammad Ibtsam - PharmDNoch keine Bewertungen
- PharmacoeconomicsDokument35 SeitenPharmacoeconomicsMuhammad Aleem Ijaz67% (3)
- Rascati Untuk Kuliah Chapter 2Dokument16 SeitenRascati Untuk Kuliah Chapter 2DALI SAPARI 2021Noch keine Bewertungen
- The Role of Economic Evaluation and Priority Setting in Health Care Decision MakingDokument47 SeitenThe Role of Economic Evaluation and Priority Setting in Health Care Decision MakingiremNoch keine Bewertungen
- Tools of Health Economics PDFDokument53 SeitenTools of Health Economics PDFAdnan RahatNoch keine Bewertungen
- Ch2 Measuring and Estimating CostsDokument20 SeitenCh2 Measuring and Estimating CostsAhmad MakhloufNoch keine Bewertungen
- Pharmacoeconomics FinalDokument62 SeitenPharmacoeconomics FinalYash SoniNoch keine Bewertungen
- Chapter 5 Cost-Benefit Analysis (CBA)Dokument30 SeitenChapter 5 Cost-Benefit Analysis (CBA)Fuad AbanuraNoch keine Bewertungen
- Far Mako EconomicDokument9 SeitenFar Mako EconomicAlfix AnugrahNoch keine Bewertungen
- Pharmaco EconomicsDokument49 SeitenPharmaco EconomicsSunil100% (1)
- Outcomes Evaluation of Pharmacy Operations: Created byDokument37 SeitenOutcomes Evaluation of Pharmacy Operations: Created byShiela Marie Briones Aguila100% (1)
- Health Economics 2013Dokument42 SeitenHealth Economics 2013Syuraih AbdullahNoch keine Bewertungen
- Introduction PharmacoeconomicDokument16 SeitenIntroduction Pharmacoeconomic2013SecB100% (2)
- Economic Evaluation in Health CareDokument82 SeitenEconomic Evaluation in Health CareyihalemNoch keine Bewertungen
- Tinpus FarmakoekonomiDokument6 SeitenTinpus FarmakoekonomiYesi Widya IswariNoch keine Bewertungen
- Economics 1Dokument9 SeitenEconomics 1ayesha baberNoch keine Bewertungen
- 3.3.1 Medical Care and Administration: Charges vs. CostsDokument5 Seiten3.3.1 Medical Care and Administration: Charges vs. CostsmarlinNoch keine Bewertungen
- 8 - Real Life HTADokument34 Seiten8 - Real Life HTAgunanti1307Noch keine Bewertungen
- Commed - Economics in Health Care 08Dokument51 SeitenCommed - Economics in Health Care 08api-3856051100% (1)
- HECO U4 - Eco EvaluationDokument107 SeitenHECO U4 - Eco EvaluationMikee MeladNoch keine Bewertungen
- Podcast IIDokument49 SeitenPodcast IINumeratorNoch keine Bewertungen
- Uro EthicsDokument36 SeitenUro EthicsHafizur RashidNoch keine Bewertungen
- L4 AsimDokument27 SeitenL4 Asimaleen qawareetNoch keine Bewertungen
- Basics of Pharmacoeconomics and Outcomes ResearchDokument48 SeitenBasics of Pharmacoeconomics and Outcomes Researchadrianne_apsNoch keine Bewertungen
- Chapter 9. Pharmacoeconomics and Economic Evaluation of Drug TherapiesDokument9 SeitenChapter 9. Pharmacoeconomics and Economic Evaluation of Drug TherapiesJuan AntonioNoch keine Bewertungen
- Pharmacoeconomic ConsiderationDokument17 SeitenPharmacoeconomic ConsiderationAnisha PandeyNoch keine Bewertungen
- Foundation Issues: Pharmacoeconomics: Principles, Methods, and ApplicationsDokument16 SeitenFoundation Issues: Pharmacoeconomics: Principles, Methods, and ApplicationsbencleeseNoch keine Bewertungen
- Module 6-Key Attributes of Cost AnalysesDokument3 SeitenModule 6-Key Attributes of Cost AnalysesLou CalderonNoch keine Bewertungen
- Health Affairs Blog Appropriate Use of Reference Pricing Can Increase Value PrintDokument5 SeitenHealth Affairs Blog Appropriate Use of Reference Pricing Can Increase Value PrintBrett BernsteinNoch keine Bewertungen
- Chapter 01Dokument14 SeitenChapter 01flaviamarottaNoch keine Bewertungen
- Health Technnology Assessment Module3Dokument4 SeitenHealth Technnology Assessment Module3jenkenny00sNoch keine Bewertungen
- Health EconomicsDokument46 SeitenHealth EconomicsSmitha Reni100% (2)
- Basics of Pharmacoeconomics and Outcomes ResearchDokument48 SeitenBasics of Pharmacoeconomics and Outcomes ResearchArvind NagNoch keine Bewertungen
- GP 6Dokument31 SeitenGP 6maggimanojNoch keine Bewertungen
- Principles of Costs and CostingDokument50 SeitenPrinciples of Costs and CostingSOOMA OSMANNoch keine Bewertungen
- Appropriate Use of Reference Pricing CanDokument5 SeitenAppropriate Use of Reference Pricing CansunnyNoch keine Bewertungen
- What Is Value-Based Healthcare - NEJM CatalystDokument3 SeitenWhat Is Value-Based Healthcare - NEJM CatalystRémi DANHOUNDONoch keine Bewertungen
- 3.outcome AnalyzeDokument29 Seiten3.outcome AnalyzeMunawar ReyhanNoch keine Bewertungen
- الاقتصاديه مترجمDokument23 Seitenالاقتصاديه مترجمأسماء المخلافيNoch keine Bewertungen
- Resource AllocationDokument17 SeitenResource AllocationkarynaNoch keine Bewertungen
- Future Directions For Client Education (H.e)Dokument14 SeitenFuture Directions For Client Education (H.e)Trina Joy Domantay80% (5)
- 1 - 4 Quality of CareDokument10 Seiten1 - 4 Quality of CareRaul Gascueña100% (1)
- Five Cost of IllnessDokument10 SeitenFive Cost of Illnessenas.aborayaNoch keine Bewertungen
- Pharmacoeconomics: Pharmacoeconomics Has Been Defined As The Description and The Analysis of The Cost of Drug TherapyDokument6 SeitenPharmacoeconomics: Pharmacoeconomics Has Been Defined As The Description and The Analysis of The Cost of Drug TherapySreya SanilNoch keine Bewertungen
- Organization of Health Insurance MarketsDokument27 SeitenOrganization of Health Insurance MarketsAndrie FaisalNoch keine Bewertungen
- Types of Economic and Humanistic Outcomes AssessmentsDokument47 SeitenTypes of Economic and Humanistic Outcomes AssessmentsPharmacotherapyNoch keine Bewertungen
- Rights and Responsibilities in Behavioral Healthcare: For Clinical Social Workers, Consumers, and Third PartiesVon EverandRights and Responsibilities in Behavioral Healthcare: For Clinical Social Workers, Consumers, and Third PartiesNoch keine Bewertungen
- Textbook of Urgent Care Management: Chapter 42, Evaluation and Management of Coding and DocumentationVon EverandTextbook of Urgent Care Management: Chapter 42, Evaluation and Management of Coding and DocumentationNoch keine Bewertungen
- My Research Proposal Final (AI)Dokument4 SeitenMy Research Proposal Final (AI)Abû Säleh ShipónNoch keine Bewertungen
- Wolfe - Understanding and Treating Anxiety Disorders An Integrative Approach To Healing The Wounded Self (2005)Dokument300 SeitenWolfe - Understanding and Treating Anxiety Disorders An Integrative Approach To Healing The Wounded Self (2005)Ruxandra Pop100% (5)
- Exercise No. 3 Hospital FormularyDokument5 SeitenExercise No. 3 Hospital Formularyheyyo ggNoch keine Bewertungen
- PSYCHOANALYSISDokument30 SeitenPSYCHOANALYSISRia de los SantosNoch keine Bewertungen
- Dispensing Poster A4Dokument1 SeiteDispensing Poster A4TuxillNoch keine Bewertungen
- 1320-Doctors in Sweden Say There Is A Cure For ArthritisDokument5 Seiten1320-Doctors in Sweden Say There Is A Cure For Arthritisguapo210% (1)
- List of Colleges Granted Letter of Permission (LOP) To Establish New Ayurveda Colleges From The A.Y. 2022-23 Till 27.12.2022Dokument3 SeitenList of Colleges Granted Letter of Permission (LOP) To Establish New Ayurveda Colleges From The A.Y. 2022-23 Till 27.12.2022Pranjal Shrivastav100% (1)
- Chapter 15 - Multiple ChoiceDokument12 SeitenChapter 15 - Multiple ChoiceNicky PhakathiNoch keine Bewertungen
- Json Definitivo Label RXDokument3 SeitenJson Definitivo Label RXAnderson Manuel Marquez NuñezNoch keine Bewertungen
- White LabelDokument1 SeiteWhite LabelJb Cano ManriqueNoch keine Bewertungen
- Musicophilia Tales of Music and The BrainDokument3 SeitenMusicophilia Tales of Music and The BrainClark's Eye on Books0% (1)
- Yalom, I.D - 2020 - The Theory and Practice of Group Psychotherapy-22-61Dokument40 SeitenYalom, I.D - 2020 - The Theory and Practice of Group Psychotherapy-22-61Máthé AdriennNoch keine Bewertungen
- Dialog Bahasa InggirsDokument2 SeitenDialog Bahasa InggirsKeRtha NeghaRaNoch keine Bewertungen
- Drama TherapyDokument22 SeitenDrama TherapyJayanth Mamundi0% (1)
- Daftar Obat High Alert MedicationDokument7 SeitenDaftar Obat High Alert Medicationlala bestgirlNoch keine Bewertungen
- General Pharmacology (2) - 1Dokument248 SeitenGeneral Pharmacology (2) - 1Irumvamwizerwa OnesmeNoch keine Bewertungen
- Wiki Therepeutic Vax (No BS)Dokument4 SeitenWiki Therepeutic Vax (No BS)Jack NestelroadNoch keine Bewertungen
- Dr. Jarir at Thobari, PHD - Basic Pharmacovigilance PDFDokument35 SeitenDr. Jarir at Thobari, PHD - Basic Pharmacovigilance PDFFerina AngeliaNoch keine Bewertungen
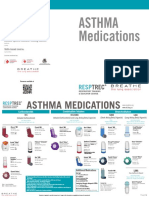
- Courses Offered:: Asthma MedicationsDokument2 SeitenCourses Offered:: Asthma MedicationsM Naeem ArhamNoch keine Bewertungen
- Competences Required For Effective Systemic TherapiesDokument27 SeitenCompetences Required For Effective Systemic TherapiesJosé BernalNoch keine Bewertungen
- CNL-500 Topic 6: Comparison WorksheetDokument6 SeitenCNL-500 Topic 6: Comparison WorksheetDeekay100% (23)
- Play TherapyDokument26 SeitenPlay TherapypastellarNoch keine Bewertungen
- Dompy Tablet & Susp Patient Information LeafletDokument1 SeiteDompy Tablet & Susp Patient Information Leafletpharmacia1.com100% (1)
- 10 - Cognitive TherapyDokument32 Seiten10 - Cognitive TherapymartinjeanellNoch keine Bewertungen
- Complementary and Alternative TherapiesDokument23 SeitenComplementary and Alternative Therapiesishicaa100% (1)
- Module 5 PEDokument28 SeitenModule 5 PEGauri GhuleNoch keine Bewertungen
- Jsap 12633Dokument6 SeitenJsap 12633Getahun TeshomeNoch keine Bewertungen
- Cognitive-Behavioral Therapy Plus Hypnosis For Distress During Breast Radiotherapy: A Randomized TrialDokument15 SeitenCognitive-Behavioral Therapy Plus Hypnosis For Distress During Breast Radiotherapy: A Randomized TrialIonela BărbosNoch keine Bewertungen
- Reality, Gestalt and Solution-Focused TherapyDokument24 SeitenReality, Gestalt and Solution-Focused TherapyMimi Generous100% (4)
- VAL-SV-E0163-P PCBA Depanelization Router Elite Machine Validation Plan - Edy-29 Nov (CK)Dokument8 SeitenVAL-SV-E0163-P PCBA Depanelization Router Elite Machine Validation Plan - Edy-29 Nov (CK)arumNoch keine Bewertungen