Das könnte Ihnen auch gefallen
- Reverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)Von EverandReverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)Noch keine Bewertungen
- Cardio MyopathiesDokument39 SeitenCardio Myopathiesinyanji.barasaNoch keine Bewertungen
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisVon EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisBewertung: 5 von 5 Sternen5/5 (1)
- AtherosclerosisDokument65 SeitenAtherosclerosisAmanuel MaruNoch keine Bewertungen
- Arteriosclerosis With Special Emphasis On Atherosclerosis: Pre-Reading: Robbins Basic Pathology 9th Ed: Pages 335-343Dokument49 SeitenArteriosclerosis With Special Emphasis On Atherosclerosis: Pre-Reading: Robbins Basic Pathology 9th Ed: Pages 335-343mus zaharaNoch keine Bewertungen
- Ischemic Heart DiseaseDokument39 SeitenIschemic Heart DiseaserahulbafnaeNoch keine Bewertungen
- Atherosclerosis 2 2017 (Modified)Dokument64 SeitenAtherosclerosis 2 2017 (Modified)Remo B AbyNoch keine Bewertungen
- Diseases of The Heart Part 1Dokument141 SeitenDiseases of The Heart Part 1Amanuel MaruNoch keine Bewertungen
- CVS NotesDokument26 SeitenCVS NotesKelly YeowNoch keine Bewertungen
- Cardiovascular DentDokument92 SeitenCardiovascular DentVincent De AsisNoch keine Bewertungen
- ASCVDDokument64 SeitenASCVDgalemayehu471Noch keine Bewertungen
- Ischaemic Heart DiseaseDokument66 SeitenIschaemic Heart DiseaseImtiyazNoch keine Bewertungen
- 5 - Pathology of CADDokument58 Seiten5 - Pathology of CADregeti bhargavNoch keine Bewertungen
- CardiomyopathyDokument27 SeitenCardiomyopathyakoeljames8543Noch keine Bewertungen
- Ischaemic Heart DiseaseDokument25 SeitenIschaemic Heart DiseaseKelvinTMaikanaNoch keine Bewertungen
- SBCP - Cardiovascular PathologyDokument11 SeitenSBCP - Cardiovascular PathologyAndrew EldeiryNoch keine Bewertungen
- Cardiovascular Pathology 2024Dokument132 SeitenCardiovascular Pathology 2024Chen HouyuNoch keine Bewertungen
- Cagayan State University College of Medicine and Surgery SY: 2009-2010Dokument41 SeitenCagayan State University College of Medicine and Surgery SY: 2009-2010ahmad usmanNoch keine Bewertungen
- Peny. KardiovaskulerDokument99 SeitenPeny. Kardiovaskulerpraptiningsih.90Noch keine Bewertungen
- Cardiovascular Patho 1 OgenaDokument87 SeitenCardiovascular Patho 1 OgenaQuolette ConstanteNoch keine Bewertungen
- AterosklerosisDokument40 SeitenAterosklerosisIda Benecia DeseNoch keine Bewertungen
- ATHEROSCLEROSISDokument41 SeitenATHEROSCLEROSISDoc On CallNoch keine Bewertungen
- Lecture 3 - IHDDokument29 SeitenLecture 3 - IHDقاسم اليوسفيNoch keine Bewertungen
- Pathology CVS #5 by Omar BaniErshaidDokument5 SeitenPathology CVS #5 by Omar BaniErshaidبصيص اليقينNoch keine Bewertungen
- Coronary Artery Disease and Acute Coronary Syndrome Myocardial InfarctionDokument3 SeitenCoronary Artery Disease and Acute Coronary Syndrome Myocardial InfarctionsenaringNoch keine Bewertungen
- Patologi Bedah Sistem Vaskuler A Dan VDokument77 SeitenPatologi Bedah Sistem Vaskuler A Dan Vfienda feraniNoch keine Bewertungen
- The Cardiovascular SystemDokument43 SeitenThe Cardiovascular Systemtravis efraimNoch keine Bewertungen
- Cardiovascular Physio Logic ProcessDokument35 SeitenCardiovascular Physio Logic ProcessmatrixtrinityNoch keine Bewertungen
- 4 - Patophysiology of Cardiovascular Disease PPDokument126 Seiten4 - Patophysiology of Cardiovascular Disease PPFirdaws FaxirNoch keine Bewertungen
- AtherosclerosisDokument41 SeitenAtherosclerosisSachin KumarNoch keine Bewertungen
- 4th Auguest 2016 Fluid and Hemodynamic Disorders 2011Dokument81 Seiten4th Auguest 2016 Fluid and Hemodynamic Disorders 2011Majkel Benche Custodio MllNoch keine Bewertungen
- Biology: ALBG10: Topic 1: Lifestyle, Health and Risk CVD & AtherosclerosisDokument46 SeitenBiology: ALBG10: Topic 1: Lifestyle, Health and Risk CVD & AtherosclerosisNuraina SakinaNoch keine Bewertungen
- WINSEM2019-20 BIT1026 TH VL2019205006678 Reference Material I 28-Jan-2020 Atherosclerosis-28 JANDokument21 SeitenWINSEM2019-20 BIT1026 TH VL2019205006678 Reference Material I 28-Jan-2020 Atherosclerosis-28 JANsubramanianNoch keine Bewertungen
- Hemodynamic PathologyDokument9 SeitenHemodynamic PathologyjoeNoch keine Bewertungen
- Hemodynamic Disorders: BY Dr. Birhane H (MD)Dokument88 SeitenHemodynamic Disorders: BY Dr. Birhane H (MD)Biruck BirhanuNoch keine Bewertungen
- Lecture 18 - ThrombosisDokument32 SeitenLecture 18 - Thrombosisapi-3703352100% (2)
- AtherosclerosisDokument36 SeitenAtherosclerosisjainilNoch keine Bewertungen
- PATHO-II Unit V Cardiovascular DisordersDokument52 SeitenPATHO-II Unit V Cardiovascular DisordersMuhammad ShayanNoch keine Bewertungen
- Lec10 CV PathologyDokument75 SeitenLec10 CV PathologymanuelNoch keine Bewertungen
- Cvs BCMDokument117 SeitenCvs BCMjaniceli0207Noch keine Bewertungen
- Myocardial InfarctionDokument19 SeitenMyocardial InfarctionkiflomNoch keine Bewertungen
- Thrombosis: Thrombus Is Blood That Has Clotted in The Heart or A Blood VesselDokument53 SeitenThrombosis: Thrombus Is Blood That Has Clotted in The Heart or A Blood VesselhjjhNoch keine Bewertungen
- Patho 2Dokument131 SeitenPatho 2ademabdellaaleNoch keine Bewertungen
- Myocardial InfarctionDokument20 SeitenMyocardial Infarction* mokhtar !!50% (2)
- Ischemic Heart Disease (IHD)Dokument70 SeitenIschemic Heart Disease (IHD)Deborah AnnNoch keine Bewertungen
- Cardiovascular Study GuideDokument19 SeitenCardiovascular Study GuideLouise FraserNoch keine Bewertungen
- Notes (1 To 6)Dokument21 SeitenNotes (1 To 6)Justin EvansNoch keine Bewertungen
- Non Modifiable FactorsDokument2 SeitenNon Modifiable FactorsColette Marie PerezNoch keine Bewertungen
- Patologi Pembuluh DarahDokument77 SeitenPatologi Pembuluh DarahDenise JohnsonNoch keine Bewertungen
- SHOCK DiscussionDokument22 SeitenSHOCK DiscussionNavpreet Kaur100% (1)
- Hemodynamic Disorder PC1Dokument227 SeitenHemodynamic Disorder PC1Bereket weybaNoch keine Bewertungen
- نسخة HeartDokument29 Seitenنسخة HeartKyunaNoch keine Bewertungen
- Cardiovascular PathologyDokument182 SeitenCardiovascular PathologyPavan chowdaryNoch keine Bewertungen
- Cerebrovascular Disease and Coronary Artery Disease: DR Masona-MutitiDokument28 SeitenCerebrovascular Disease and Coronary Artery Disease: DR Masona-MutitiShaun MazorodzeNoch keine Bewertungen
- Chapter 13Dokument7 SeitenChapter 13newmexicoomfsNoch keine Bewertungen
- VNSG 1409 - Exam 3Dokument24 SeitenVNSG 1409 - Exam 3luna nguyenNoch keine Bewertungen
- 11.sudden Natural Death 3Dokument55 Seiten11.sudden Natural Death 3Hasabo AwadNoch keine Bewertungen
- Clase Cardiopatia IsquémicaDokument132 SeitenClase Cardiopatia IsquémicaSusy OcampoNoch keine Bewertungen
- Cardiovascular System Pathology, MBCHBDokument18 SeitenCardiovascular System Pathology, MBCHBSecret AgentNoch keine Bewertungen
- Vascular Disorder: DR Nur Asyilla Che Jalil Pathology Department PPSP HusmDokument140 SeitenVascular Disorder: DR Nur Asyilla Che Jalil Pathology Department PPSP HusmHaziq KamardinNoch keine Bewertungen
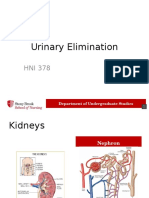
- Urinary Elimination 2014 VoiceDokument32 SeitenUrinary Elimination 2014 VoiceMohammad Usman QureshiNoch keine Bewertungen
- Abiera - Effect of NP Discharge On 30 Day Hospital Readmission This One 4-29-2015 This One.Dokument14 SeitenAbiera - Effect of NP Discharge On 30 Day Hospital Readmission This One 4-29-2015 This One.Mohammad Usman QureshiNoch keine Bewertungen
- Phlebotomy Review Shee1Dokument8 SeitenPhlebotomy Review Shee1Mohammad Usman Qureshi100% (1)
- Proof For Sadl-Maliki FiqhDokument7 SeitenProof For Sadl-Maliki FiqhMohammad Usman QureshiNoch keine Bewertungen
- Proof For Sadl-Maliki FiqhDokument7 SeitenProof For Sadl-Maliki FiqhMohammad Usman QureshiNoch keine Bewertungen
- Allergic Reaction ManagementDokument2 SeitenAllergic Reaction ManagementMohammad Usman QureshiNoch keine Bewertungen
- Bob Page 12 Lead ECG-Capnongraphy ClassesDokument1 SeiteBob Page 12 Lead ECG-Capnongraphy ClassesMohammad Usman QureshiNoch keine Bewertungen
- Test QuestionsDokument14 SeitenTest QuestionsMohammad Usman QureshiNoch keine Bewertungen
- To Be or To Derrida. The Abdication of MeaningDokument5 SeitenTo Be or To Derrida. The Abdication of MeaningMohammad Usman QureshiNoch keine Bewertungen
- Certificate of Completion: Jaclyn CappielloDokument1 SeiteCertificate of Completion: Jaclyn CappielloMohammad Usman QureshiNoch keine Bewertungen
- Mishkat Al Anwar by Imam Al GhazaliDokument91 SeitenMishkat Al Anwar by Imam Al GhazaliMohammad Usman Qureshi100% (2)
- Heart Attacks Reported Following Covid VaccineDokument64 SeitenHeart Attacks Reported Following Covid VaccineJosh SingerNoch keine Bewertungen
- Ninja NerdDokument3 SeitenNinja NerdSalsabila HMNoch keine Bewertungen
- Cardiovascular System Diseases Part 1Dokument22 SeitenCardiovascular System Diseases Part 1Prince Rener Velasco PeraNoch keine Bewertungen
- Newborn Adaptation Assessment 2013 FINALDokument21 SeitenNewborn Adaptation Assessment 2013 FINALJennNoch keine Bewertungen
- Fallot TetralogyDokument20 SeitenFallot Tetralogykgt88Noch keine Bewertungen
- Physiological Indicators: Heart Rate Rate of Perceived Exertion PacingDokument29 SeitenPhysiological Indicators: Heart Rate Rate of Perceived Exertion PacingAlyssa AlejandroNoch keine Bewertungen
- Hypertension Health ChallengeDokument19 SeitenHypertension Health ChallengeElijah Tochukwu DavidNoch keine Bewertungen
- Electric Alex 519171918 GernDokument950 SeitenElectric Alex 519171918 GernShyamSoniNoch keine Bewertungen
- Ebook First Aid For The Pediatrics Clerkship 4E True PDF Full Chapter PDFDokument67 SeitenEbook First Aid For The Pediatrics Clerkship 4E True PDF Full Chapter PDFgwendolyn.jordan283100% (26)
- Ultrasound in Anaesthesia and Intensive Care - College of (PDFDrive)Dokument71 SeitenUltrasound in Anaesthesia and Intensive Care - College of (PDFDrive)Tabish JavaidNoch keine Bewertungen
- Fitness Exercises: Cardiorespiratory and Muscular Fitness: ObjectivesDokument16 SeitenFitness Exercises: Cardiorespiratory and Muscular Fitness: ObjectivesArabella Grace AcibarNoch keine Bewertungen
- Fluid Responsiveness in Mechanically Ventilated Patients A Review of Indices Used in Intensive CADokument9 SeitenFluid Responsiveness in Mechanically Ventilated Patients A Review of Indices Used in Intensive CAerwanNoch keine Bewertungen
- Case History: Year 8 SemesterDokument26 SeitenCase History: Year 8 SemesterNarmada PemathilakaNoch keine Bewertungen
- Fluid and Electrolyte ChartDokument1 SeiteFluid and Electrolyte ChartJenny Varghese100% (1)
- Acute Myocardial InfarctionDokument62 SeitenAcute Myocardial InfarctionJohn Alvin YoroNoch keine Bewertungen
- Fundamentals of Body CT 5th EdDokument415 SeitenFundamentals of Body CT 5th EdRuxandra TartaNoch keine Bewertungen
- 2010 Ieee Titb OreskoDokument7 Seiten2010 Ieee Titb OreskoPedro ContrerasNoch keine Bewertungen
- Lesson Plan Phy 1114 202201Dokument4 SeitenLesson Plan Phy 1114 202201IdzhamReezaNoch keine Bewertungen
- Effects of Endotoxin On Pacemaker Funny Current in Hek 293 CellsDokument190 SeitenEffects of Endotoxin On Pacemaker Funny Current in Hek 293 CellsNemo SecretNoch keine Bewertungen
- Cardiac & Respiratory Diseases in PregnancyDokument30 SeitenCardiac & Respiratory Diseases in PregnancyKerod AbebeNoch keine Bewertungen
- Inside My BodyDokument72 SeitenInside My Bodyumm_aasiyaNoch keine Bewertungen
- Project 4.4.2: Heart Disease Interventions - Principles of BiomedicalDokument6 SeitenProject 4.4.2: Heart Disease Interventions - Principles of BiomedicalMATTHEW DIAZNoch keine Bewertungen
- Lesson Plan in Biology For Science VIIDokument3 SeitenLesson Plan in Biology For Science VIIJonah Mae Bilaos-BielNoch keine Bewertungen
- Coronary Microvascular Disease Pathogenic Mechanisms and Therapeutic OptionsDokument17 SeitenCoronary Microvascular Disease Pathogenic Mechanisms and Therapeutic OptionsZuleynny TellesNoch keine Bewertungen
- Acsms Resources For The Exercise Physiologist 2nd Edition Ebook PDFDokument61 SeitenAcsms Resources For The Exercise Physiologist 2nd Edition Ebook PDFjames.keeter432100% (41)
- OxfordAQA 9201 1 Final MS Jun23 v1.0Dokument19 SeitenOxfordAQA 9201 1 Final MS Jun23 v1.0remaselshazly76Noch keine Bewertungen
- Anatomi Dan Fisiologi: The Cardiovascular SystemDokument8 SeitenAnatomi Dan Fisiologi: The Cardiovascular SystemAzrin MohayaddinNoch keine Bewertungen
- Biology: Revised Syllabus For Higher Secondary First Year CourseDokument4 SeitenBiology: Revised Syllabus For Higher Secondary First Year CourseamitumikoibNoch keine Bewertungen
- 66Dokument84 Seiten66Jimmy Jimmy0% (1)
- SNC2D1 Biology Unit ReviewDokument3 SeitenSNC2D1 Biology Unit ReviewSA - 10WB 933839 The Woodlands SSNoch keine Bewertungen