Das könnte Ihnen auch gefallen
- 2300 Fall Midterm Exam Review (Lecture) - 1Dokument5 Seiten2300 Fall Midterm Exam Review (Lecture) - 1jesNoch keine Bewertungen
- Medicine List For OTDokument51 SeitenMedicine List For OTtom greg0% (1)
- Chapter 4 - Reproductive Health NotesDokument5 SeitenChapter 4 - Reproductive Health NotesShagufta100% (1)
- Thesis Protocol: DR - Manali Kagathara Narayanamultispeciality Hospital, JaipurDokument15 SeitenThesis Protocol: DR - Manali Kagathara Narayanamultispeciality Hospital, JaipurMaitree PNoch keine Bewertungen
- DRTP Sample QuestionsDokument6 SeitenDRTP Sample QuestionsDeepthi SreenivasNoch keine Bewertungen
- DDX of RIF Mass (Syazwani)Dokument44 SeitenDDX of RIF Mass (Syazwani)Nurul Syazwani RamliNoch keine Bewertungen
- Tirzepatide Significantly Reduced A1C and Body Weight in People With Type 2 Diabetes in Two Phase 3 Trials From Lilly's SURPASS ProgramDokument4 SeitenTirzepatide Significantly Reduced A1C and Body Weight in People With Type 2 Diabetes in Two Phase 3 Trials From Lilly's SURPASS ProgramJOSÉ CARLOS ÁLVAREZ PAYARESNoch keine Bewertungen
- Final Update On Antenatal Steroids - DR PadmeshDokument66 SeitenFinal Update On Antenatal Steroids - DR PadmeshAhalia NicuNoch keine Bewertungen
- Chitoglucan New OverviewDokument6 SeitenChitoglucan New OverviewmjmorcelliNoch keine Bewertungen
- Dyspepsia: Dr. Arif Nur Widodo SP - PDDokument31 SeitenDyspepsia: Dr. Arif Nur Widodo SP - PDMonica Kristina HutabaratNoch keine Bewertungen
- SAR PPT 1-Program - 07Dokument36 SeitenSAR PPT 1-Program - 07ni60Noch keine Bewertungen
- Management of Acute MalnutritionDokument64 SeitenManagement of Acute MalnutritionDO or DIENoch keine Bewertungen
- NUT 116BL Major Case Study Critical IllnessDokument10 SeitenNUT 116BL Major Case Study Critical IllnessAkarin Mittongtare100% (1)
- Case Study #3 Renal 1. LabDokument9 SeitenCase Study #3 Renal 1. LabLindrit AliuNoch keine Bewertungen
- Preterm+Prelabour+Rupture+of+the+Membranes Sept2015Dokument12 SeitenPreterm+Prelabour+Rupture+of+the+Membranes Sept2015molenNoch keine Bewertungen
- Microbiology & Immunology - Topical Past Papers-1 PDFDokument32 SeitenMicrobiology & Immunology - Topical Past Papers-1 PDFArooba Khalid100% (1)
- Ptl/Pprom and Multifetal Gestation: Anna Buabbud MD Ms3 LectureDokument38 SeitenPtl/Pprom and Multifetal Gestation: Anna Buabbud MD Ms3 LectureNik C0% (1)
- Obs UM Paper 2Dokument16 SeitenObs UM Paper 2Muhammad Abbas AliNoch keine Bewertungen
- Palliative EnciesDokument96 SeitenPalliative EnciesnandanNoch keine Bewertungen
- Presentation Thyroid ScanDokument20 SeitenPresentation Thyroid ScanMuhammad Safwan Ahmad FadzilNoch keine Bewertungen
- CC C C: June 8, 2011 By: Santos, Edilberto DBDokument63 SeitenCC C C: June 8, 2011 By: Santos, Edilberto DBHakugeiNoch keine Bewertungen
- Misoprostol Dosage Recommendations 2012 4Dokument1 SeiteMisoprostol Dosage Recommendations 2012 4Bonifacius Bayu Erlangga KusumaNoch keine Bewertungen
- Clinical Guideline: Prelabour Rupture of The Membranes (PROM) 37 Weeks Clinical GuidelineDokument10 SeitenClinical Guideline: Prelabour Rupture of The Membranes (PROM) 37 Weeks Clinical GuidelineUtomo BudidarmoNoch keine Bewertungen
- Management of CA Vulva 2Dokument33 SeitenManagement of CA Vulva 2api-3705046Noch keine Bewertungen
- MCQs Term 2 Test 2022 - After Post HocDokument16 SeitenMCQs Term 2 Test 2022 - After Post HocRuqaeya SaqibNoch keine Bewertungen
- IKD5 - Interventional Uro-Radiology - Current Practices and Aspirations in MauritiusDokument81 SeitenIKD5 - Interventional Uro-Radiology - Current Practices and Aspirations in MauritiusRenal Association MauritiusNoch keine Bewertungen
- Body Weight in TBDokument8 SeitenBody Weight in TBNiar MarhaliNoch keine Bewertungen
- Syllabus For BPKMCH NEPALDokument7 SeitenSyllabus For BPKMCH NEPALDeep SharmaNoch keine Bewertungen
- Mompati Letsweletse Hiv Case 20110183Dokument25 SeitenMompati Letsweletse Hiv Case 20110183Mompati LetsweletseNoch keine Bewertungen
- Table 4.1 AFS Classifi Cation System (: The Embryological-Clinical Classifi CationDokument111 SeitenTable 4.1 AFS Classifi Cation System (: The Embryological-Clinical Classifi CationArya Syafaromania RachmaNoch keine Bewertungen
- Https Tdiagnostics - Telangana.gov - in ViewFiles - Aspx ReportId HK9UQ4C5ZEZ7ICEuNXmyPwDokument8 SeitenHttps Tdiagnostics - Telangana.gov - in ViewFiles - Aspx ReportId HK9UQ4C5ZEZ7ICEuNXmyPwKuncham LakshmiNoch keine Bewertungen
- 002 Intrapartum Fetal Heart Rate Monitoring 3a - ACOG Bulletin 106 PDFDokument11 Seiten002 Intrapartum Fetal Heart Rate Monitoring 3a - ACOG Bulletin 106 PDFale_fearNoch keine Bewertungen
- Viva QuestionsDokument2 SeitenViva QuestionsSanket TelangNoch keine Bewertungen
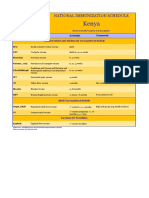
- Kenya Immunization ScheduleDokument1 SeiteKenya Immunization ScheduleDani AnyikaNoch keine Bewertungen
- FOB Transferrin+Calprotectin Lactoferrin Combo CardDokument2 SeitenFOB Transferrin+Calprotectin Lactoferrin Combo CardEyad KatrangiNoch keine Bewertungen
- MCQ PDF 5 PDFDokument3 SeitenMCQ PDF 5 PDFshakeelNoch keine Bewertungen
- Chapter 40: Gastrointestinal Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDokument6 SeitenChapter 40: Gastrointestinal Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNoch keine Bewertungen
- Refresh Pathology 3rd Ed. 2022-Dr. Shiva MDDokument220 SeitenRefresh Pathology 3rd Ed. 2022-Dr. Shiva MD147-haricharan voduri100% (1)
- Perioperative Chemotherapy (Neoadjuvant or Adjuvant)Dokument4 SeitenPerioperative Chemotherapy (Neoadjuvant or Adjuvant)c.ramNoch keine Bewertungen
- B Lynch PDFDokument1 SeiteB Lynch PDFPradana ACNoch keine Bewertungen
- Triple Negative Breast Cancer, Experience of Military Hospital Rabat: About 52 CasesDokument10 SeitenTriple Negative Breast Cancer, Experience of Military Hospital Rabat: About 52 CasesIJAR JOURNALNoch keine Bewertungen
- USNI Medication TestDokument8 SeitenUSNI Medication Testusni100% (31)
- Y3b3 Ong Groupd B - 13Dokument15 SeitenY3b3 Ong Groupd B - 13Akmal ZaimNoch keine Bewertungen
- Octaseeds Rise Review Posttest Compilation 120qDokument19 SeitenOctaseeds Rise Review Posttest Compilation 120qAngela Saldajeno100% (3)
- A Study On Acute Surgical Abdomen in Paediatric Age Group: Original Research ArticleDokument5 SeitenA Study On Acute Surgical Abdomen in Paediatric Age Group: Original Research ArticleApple IdeaNoch keine Bewertungen
- Laparoscopic Management of Malignant Ovarian Cysts: A 7 Se National Survey. Part 2: Follow-Up and Final TreatmentDokument4 SeitenLaparoscopic Management of Malignant Ovarian Cysts: A 7 Se National Survey. Part 2: Follow-Up and Final TreatmentAgustin LindaNoch keine Bewertungen
- Vol. 229, No. 4S2, October 2019 Scientific Poster Presentations E69Dokument2 SeitenVol. 229, No. 4S2, October 2019 Scientific Poster Presentations E69Mateo TamayoNoch keine Bewertungen
- Abdominal Pain - Parietal or VisceralDokument1 SeiteAbdominal Pain - Parietal or Viscerallimaihwa1990Noch keine Bewertungen
- Question 1 of 35Dokument130 SeitenQuestion 1 of 35Ahmed SamirNoch keine Bewertungen
- Mucinous Neoplasm of Appendix TreatmentDokument3 SeitenMucinous Neoplasm of Appendix TreatmentInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- CholeL During BariatricDokument6 SeitenCholeL During BariatriclucasakrNoch keine Bewertungen
- Ray Coquard2018Dokument26 SeitenRay Coquard2018Juan Daniel Serrano GuerreroNoch keine Bewertungen
- 17-09-2019 Lower GI FINALDokument32 Seiten17-09-2019 Lower GI FINALNaima HabibNoch keine Bewertungen
- 139-Article Text-416-1-10-20180204Dokument3 Seiten139-Article Text-416-1-10-20180204Kriti KumariNoch keine Bewertungen
- Imaging AppendicitisDokument75 SeitenImaging AppendicitiswilandayuNoch keine Bewertungen
- BORRESDokument3 SeitenBORRESMonique BorresNoch keine Bewertungen
- 1.2.2. Emergency Abdominal ImagingDokument51 Seiten1.2.2. Emergency Abdominal ImagingNoura AdzmiaNoch keine Bewertungen
- Annals of Medicine and Surgery: Case ReportDokument4 SeitenAnnals of Medicine and Surgery: Case ReportDimas ErlanggaNoch keine Bewertungen
- Dysphagia and Weight Loss in A Middle-Aged Man: ProblemDokument9 SeitenDysphagia and Weight Loss in A Middle-Aged Man: ProblemEstellaNoch keine Bewertungen
- Gossypiboma Case ReportDokument2 SeitenGossypiboma Case ReportArvind KushwahaNoch keine Bewertungen
- Carpio CalaycayDokument4 SeitenCarpio CalaycayCzara DyNoch keine Bewertungen
- Fetal Assessment and Wellbeing in Pregnancy (FetalDokument23 SeitenFetal Assessment and Wellbeing in Pregnancy (Fetalapi-3705046100% (1)
- CTGDokument20 SeitenCTGjaya ruban100% (1)
- Chronic Kidney Disease and The Involvement of Estrogen Hormones in Its Pathogenesis and ProgressionDokument10 SeitenChronic Kidney Disease and The Involvement of Estrogen Hormones in Its Pathogenesis and Progressionshe-docNoch keine Bewertungen
- Cbahi Esr Standards PDFDokument10 SeitenCbahi Esr Standards PDFjoan olanteNoch keine Bewertungen
- Hemodynamic Case Studies: Edward G. Hamaty JR., D.O. FACCP, FACOIDokument101 SeitenHemodynamic Case Studies: Edward G. Hamaty JR., D.O. FACCP, FACOIrichard100% (1)
- Radiology of Bone TumorsDokument55 SeitenRadiology of Bone TumorsGaling Chandika PutraNoch keine Bewertungen
- Requirements1&2 POdDokument10 SeitenRequirements1&2 POdCJ AngelesNoch keine Bewertungen
- Diseases of The Hair and ScalpDokument7 SeitenDiseases of The Hair and Scalprl20Noch keine Bewertungen
- Confusion Assessment Method PDFDokument2 SeitenConfusion Assessment Method PDFAlessandro ZadraNoch keine Bewertungen
- Rise of Modern Surgery OrigiDokument46 SeitenRise of Modern Surgery OrigiPriyanka KaranamNoch keine Bewertungen
- Per Cutaneous Trans Hepatic Cholangiogram (PTC)Dokument15 SeitenPer Cutaneous Trans Hepatic Cholangiogram (PTC)Hamzeh AlmasriNoch keine Bewertungen
- Jin Gui Yao Lue Acupuncture PDFDokument2 SeitenJin Gui Yao Lue Acupuncture PDFJiayiNoch keine Bewertungen
- Inservice Surgical Hand Scrub Protocol UpdatesDokument20 SeitenInservice Surgical Hand Scrub Protocol Updatescamicam_121Noch keine Bewertungen
- Alan F. Schatzberg & Charles B. Nemeroff 01Dokument379 SeitenAlan F. Schatzberg & Charles B. Nemeroff 01Rodrigo Sanchez Lopez100% (3)
- PheochromocytomaDokument6 SeitenPheochromocytomaSonya YuNoch keine Bewertungen
- Anterior Cruciate Ligament All InsideDokument7 SeitenAnterior Cruciate Ligament All InsideVijay KumarNoch keine Bewertungen
- Acute Uterine InversionDokument6 SeitenAcute Uterine InversionBima GhovaroliyNoch keine Bewertungen
- ALGA Medical NetworkDokument56 SeitenALGA Medical NetworkCarl HernandezNoch keine Bewertungen
- Problems of The Neonate Low Birth Weight BabiesDokument25 SeitenProblems of The Neonate Low Birth Weight BabiesmelbourneichrcNoch keine Bewertungen
- Dr. SK Mathur High Flow Nasal Oxygen TherapyDokument20 SeitenDr. SK Mathur High Flow Nasal Oxygen TherapyAnish H Dave100% (1)
- ImagingDokument2 SeitenImagingFitri WirastamiNoch keine Bewertungen
- Study and Managemet of Blunt Injury AbdomenDokument128 SeitenStudy and Managemet of Blunt Injury Abdomendevireddy bruhathiNoch keine Bewertungen
- Ectopic PregnancyDokument52 SeitenEctopic Pregnancybhakta100% (2)
- ACOG Obesity in Pregnancy COREDokument15 SeitenACOG Obesity in Pregnancy CORESaranya BalamuruganNoch keine Bewertungen
- Obstetrics Case StudiesDokument5 SeitenObstetrics Case StudiesDiane AlvaradoNoch keine Bewertungen
- Shouldice CaseDokument8 SeitenShouldice CaseSolanki HalderNoch keine Bewertungen
- Human Sexual Response CycleDokument6 SeitenHuman Sexual Response CycleAbdAllah El SaydNoch keine Bewertungen
- Meera Devi - A Parivartan Self-Help Group MemberDokument2 SeitenMeera Devi - A Parivartan Self-Help Group MemberS_digitalGREENNoch keine Bewertungen
- In Patient DepartmentDokument21 SeitenIn Patient Departmentanon_663431602Noch keine Bewertungen