Das könnte Ihnen auch gefallen
- Human Papilloma VirusDokument29 SeitenHuman Papilloma Virusphone pyaeNoch keine Bewertungen
- Reflex ExercisesDokument43 SeitenReflex ExercisesFlori100% (4)
- PEDIA Review TransesDokument12 SeitenPEDIA Review TransesanonymousNoch keine Bewertungen
- 1000 English Collocations. in 10 Minutes A Day PDFDokument128 Seiten1000 English Collocations. in 10 Minutes A Day PDFMario Cesar de Oliveira100% (5)
- Case Report DifteriDokument20 SeitenCase Report DifteriKhodimatur RofiahNoch keine Bewertungen
- Family Medicine 33: 28-Year-Old Female With Dizziness: Learning ObjectivesDokument6 SeitenFamily Medicine 33: 28-Year-Old Female With Dizziness: Learning ObjectivesAndrea Kristin OrigenesNoch keine Bewertungen
- Coughs - and How To Treat ThemDokument15 SeitenCoughs - and How To Treat Themsimplybr95630% (1)
- Fungal Rhinosinusitis: Todays PresenterDokument33 SeitenFungal Rhinosinusitis: Todays Presenterimran qaziNoch keine Bewertungen
- Femina July 2020 DDokument26 SeitenFemina July 2020 DOlivia Limson DiasNoch keine Bewertungen
- Pravin Prakash P - Finalyearmsc N Navodayacollegeof NursingDokument9 SeitenPravin Prakash P - Finalyearmsc N Navodayacollegeof NursingpraywinNoch keine Bewertungen
- Refractory Anaphylaxis Algorithm 2021Dokument1 SeiteRefractory Anaphylaxis Algorithm 2021ay254Noch keine Bewertungen
- Hand Foot Mouth DiseaseDokument11 SeitenHand Foot Mouth DiseaseedelinNoch keine Bewertungen
- FNCP FormDokument7 SeitenFNCP FormRola Miranda Guiang-ManaliliNoch keine Bewertungen
- Curriculum Vitae and Sleep Apnea ProfileDokument29 SeitenCurriculum Vitae and Sleep Apnea ProfileEfri SyaifullahNoch keine Bewertungen
- Teaching Plan.Dokument13 SeitenTeaching Plan.Maria Rogine Elopre100% (2)
- RECURRENT CHRONIC COUGH GUIDEDokument24 SeitenRECURRENT CHRONIC COUGH GUIDEHameldo Andika PattinasaranyNoch keine Bewertungen
- Otitis Media: Bagian Ilmu Kesehatan THT-KL Fakultas Kedokteran Universitas Pattimura Ambon 2018Dokument2 SeitenOtitis Media: Bagian Ilmu Kesehatan THT-KL Fakultas Kedokteran Universitas Pattimura Ambon 2018Riqqah USNoch keine Bewertungen
- Thyroid DiseasesDokument76 SeitenThyroid DiseasesSolomon Fallah Foa SandyNoch keine Bewertungen
- Thyroid Disease GuideDokument65 SeitenThyroid Disease GuideIan FordeNoch keine Bewertungen
- Vitamin D Levels and Recurrent Tonsillitis in ChildrenDokument14 SeitenVitamin D Levels and Recurrent Tonsillitis in ChildrenMyarNoch keine Bewertungen
- TB MeningitisDokument11 SeitenTB MeningitisMontserrat ÁlvarezNoch keine Bewertungen
- Thyroid DiseaseDokument17 SeitenThyroid DiseaseCharlz ZipaganNoch keine Bewertungen
- Gambaran Patologi Anatomik Kelainan Sistem PernapasanDokument49 SeitenGambaran Patologi Anatomik Kelainan Sistem PernapasanWahyunitadotokaNoch keine Bewertungen
- Jurnal Edema ParuDokument54 SeitenJurnal Edema Paruindah sariNoch keine Bewertungen
- Rinitis Alergi Dan VasomotorDokument26 SeitenRinitis Alergi Dan VasomotorMardoni EfrijonNoch keine Bewertungen
- Hepatitis & It's ComplicationDokument11 SeitenHepatitis & It's ComplicationHadjar Mingfan FlamerNoch keine Bewertungen
- Relieve Cold and Flu Symptoms FastDokument4 SeitenRelieve Cold and Flu Symptoms FastDebbie beeNoch keine Bewertungen
- Bronchiolitis Guideline RecommendationsDokument10 SeitenBronchiolitis Guideline RecommendationsAmi WilliamsNoch keine Bewertungen
- Referat Kulit KakayDokument26 SeitenReferat Kulit KakayRezky Dwiputra FellanysNoch keine Bewertungen
- Larynx InfectionsDokument28 SeitenLarynx InfectionsMuskan GogiaNoch keine Bewertungen
- Diabetes Melitus: Dr. Ihsanil Husna, SPPDDokument67 SeitenDiabetes Melitus: Dr. Ihsanil Husna, SPPDnathan timothyNoch keine Bewertungen
- Hipertiroid HarrisonDokument8 SeitenHipertiroid HarrisonravenskaNoch keine Bewertungen
- Tonsilopharyngitis and Adenoid Hypertrophy in Fadhli RajifDokument1 SeiteTonsilopharyngitis and Adenoid Hypertrophy in Fadhli RajifFadhli Rajif TangkeNoch keine Bewertungen
- DRUG ERUPTION GUIDEDokument46 SeitenDRUG ERUPTION GUIDESyahDikaNoch keine Bewertungen
- Ventikular Septal Defect FixDokument18 SeitenVentikular Septal Defect FixPutri Sari DewiNoch keine Bewertungen
- Rhino PharyngitisDokument27 SeitenRhino PharyngitisinriantoNoch keine Bewertungen
- Life-Threatening Cellulitis of the Floor of the MouthDokument17 SeitenLife-Threatening Cellulitis of the Floor of the Mouthlutfia papitaNoch keine Bewertungen
- Struma Nodusa: Pembimbing: Dr. Rizapahlevi., M.Si., SP.BDokument45 SeitenStruma Nodusa: Pembimbing: Dr. Rizapahlevi., M.Si., SP.BAndre Pradnyana100% (1)
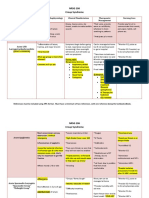
- NRSG 206 Croup SyndromeDokument3 SeitenNRSG 206 Croup SyndromeGirlwithnonameNoch keine Bewertungen
- Understanding NystagmusDokument14 SeitenUnderstanding NystagmusJefferson CaesarioNoch keine Bewertungen
- Differential Diagnosis of Rash Illness: Disease Sign/Symptoms Type of Rash Other FeaturesDokument2 SeitenDifferential Diagnosis of Rash Illness: Disease Sign/Symptoms Type of Rash Other FeaturesCarlo CondeNoch keine Bewertungen
- FFS Jambaf Aug2021Dokument2 SeitenFFS Jambaf Aug2021royescspchiitymmuaNoch keine Bewertungen
- Radiologis Gambaran Infeksi Tulang dan FrakturDokument25 SeitenRadiologis Gambaran Infeksi Tulang dan FrakturAnonymous HAbhRTs2TfNoch keine Bewertungen
- Epos Summary PDFDokument30 SeitenEpos Summary PDFPutri Rizky AmaliaNoch keine Bewertungen
- Deskripsi MurmurDokument3 SeitenDeskripsi MurmurLevina Tri RatanaNoch keine Bewertungen
- Asthma Case ReportDokument21 SeitenAsthma Case ReportbungaamiliasuariNoch keine Bewertungen
- Anatomi Dan Fisiologi HidungDokument39 SeitenAnatomi Dan Fisiologi HidungHerman YosefNoch keine Bewertungen
- Anatomy and Physiology of the ConjunctivaDokument43 SeitenAnatomy and Physiology of the ConjunctivaVincentius Okta VidiandickaNoch keine Bewertungen
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Dokument17 SeitenKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaNoch keine Bewertungen
- Serological Markers of HBV InfectionDokument8 SeitenSerological Markers of HBV InfectioncristieristiieNoch keine Bewertungen
- Antrochoanal PolypDokument18 SeitenAntrochoanal PolypReem Eshra100% (1)
- Journal Reading THT - OMADokument15 SeitenJournal Reading THT - OMAIndira MaycellaNoch keine Bewertungen
- Management of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientDokument12 SeitenManagement of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientRani Dwi NNoch keine Bewertungen
- Diabetic Foot: by Myrna Rita PMRDokument33 SeitenDiabetic Foot: by Myrna Rita PMRDianNurlitaAnggrainiNoch keine Bewertungen
- HDDokument23 SeitenHDSardjitoNoch keine Bewertungen
- Transient Thacypnea of The Newborn (TTN)Dokument6 SeitenTransient Thacypnea of The Newborn (TTN)einjhi0% (1)
- The Immune Reconstitution Inflammatory SyndromeDokument7 SeitenThe Immune Reconstitution Inflammatory SyndromeAlexandra PaunNoch keine Bewertungen
- Jurnal SinusitisDokument25 SeitenJurnal SinusitisDwi Ayu NovianaNoch keine Bewertungen
- Palmoplantar PustulosisDokument3 SeitenPalmoplantar PustulosisRobby ZayendraNoch keine Bewertungen
- Referat: Pneumonia in ElderlyDokument41 SeitenReferat: Pneumonia in Elderlyathieqah say-syahidahNoch keine Bewertungen
- Komplikasi RhinosinusitisDokument54 SeitenKomplikasi RhinosinusitisWilda Kamila SungkarNoch keine Bewertungen
- Osteonecrosis Caput FemurDokument23 SeitenOsteonecrosis Caput FemurdrhendyjuniorNoch keine Bewertungen
- Komplikasi Dan Prognosis Demam TifoidDokument6 SeitenKomplikasi Dan Prognosis Demam TifoidPundi Pandan Putri PinantiNoch keine Bewertungen
- Intestinal Coccidian ParasitesDokument23 SeitenIntestinal Coccidian ParasitesABC100% (1)
- CURRICULUM VITAE OF DENGUE EXPERTDokument59 SeitenCURRICULUM VITAE OF DENGUE EXPERTsaladass 2Noch keine Bewertungen
- Acute and Chronic Diseases of Larynx - 1 - 1Dokument60 SeitenAcute and Chronic Diseases of Larynx - 1 - 1канизаNoch keine Bewertungen
- PHARYNGITISDokument25 SeitenPHARYNGITISWesam TayaNoch keine Bewertungen
- Upper Respiratory AlterationDokument34 SeitenUpper Respiratory AlterationJulia ManaloNoch keine Bewertungen
- BronchitisDokument6 SeitenBronchitisNader Smadi100% (1)
- 03 110605e BASF API PortfolioDokument16 Seiten03 110605e BASF API PortfolioVõ Đức TrọngNoch keine Bewertungen
- Ijtk 10 (2) 227-238 PDFDokument12 SeitenIjtk 10 (2) 227-238 PDFCeline Jane DiazNoch keine Bewertungen
- 3Dokument5 Seiten3Reg ArbotanteNoch keine Bewertungen
- Yogsandesh Jan 15Dokument68 SeitenYogsandesh Jan 15rkpdmNoch keine Bewertungen
- Hall TicketDokument2 SeitenHall TicketAbhishek VaghelaNoch keine Bewertungen
- Manual For ASHA-ANMDokument42 SeitenManual For ASHA-ANMchandusgNoch keine Bewertungen
- Bacterial InfectionsDokument20 SeitenBacterial InfectionsFahad RasheedNoch keine Bewertungen
- Nutritional Perspectives For The Prevention and Mitigation of COVID-19Dokument12 SeitenNutritional Perspectives For The Prevention and Mitigation of COVID-19suci argithaNoch keine Bewertungen
- Comprehensive Health HistoryDokument1 SeiteComprehensive Health HistoryMitch GatelaNoch keine Bewertungen
- Master Ielts General Training Volume 6 Reading Practice Test 2 v9 2617055Dokument35 SeitenMaster Ielts General Training Volume 6 Reading Practice Test 2 v9 2617055daanielNoch keine Bewertungen
- Cold Breaker Like You Never Feel Any Cold Fast Relief ForDokument5 SeitenCold Breaker Like You Never Feel Any Cold Fast Relief ForPriyo NugrohoNoch keine Bewertungen
- NURSE'S DAILY DUTIESDokument13 SeitenNURSE'S DAILY DUTIESFia Nur HaryaniNoch keine Bewertungen
- Research-Evaluating Children's Health and DevelopmentDokument4 SeitenResearch-Evaluating Children's Health and Developmentdenyl ramosNoch keine Bewertungen
- Free English Practice Tests and Worksheets for Grade 7Dokument32 SeitenFree English Practice Tests and Worksheets for Grade 7vyNoch keine Bewertungen
- Biology Project: Sensory OrgansDokument50 SeitenBiology Project: Sensory OrgansAnonymous PIbP7tENNoch keine Bewertungen
- COVID 19 An Emerging Rapidly Evolving SiDokument8 SeitenCOVID 19 An Emerging Rapidly Evolving SigygyNoch keine Bewertungen
- Attitude, Knowledge, and Perception of Health Workers On Transmission and Prevention of Covid-19 in Federal Medical Centre, Birnin Kebbi, Krbbi StateDokument22 SeitenAttitude, Knowledge, and Perception of Health Workers On Transmission and Prevention of Covid-19 in Federal Medical Centre, Birnin Kebbi, Krbbi Stateakinbodewa shegxyNoch keine Bewertungen
- EverydayLife 7 Common Cold FinalDokument3 SeitenEverydayLife 7 Common Cold FinalmarisNoch keine Bewertungen
- Thi Olympic HanoiAms Khoi 10 0607Dokument2 SeitenThi Olympic HanoiAms Khoi 10 0607Long Hoang DoNoch keine Bewertungen
- Soal TTG Label N ProcedureDokument5 SeitenSoal TTG Label N ProcedureRizalMahfudinNoch keine Bewertungen