Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Case DiscussionDokument8 SeitenCase DiscussionAishwarya BharathNoch keine Bewertungen
- Chapter 1 - Psychology As A ScienceDokument21 SeitenChapter 1 - Psychology As A Sciencevarunas_250% (2)
- Healing Landscapes: Gardens As Places For Spiritual, Psychological and Physical HealingDokument49 SeitenHealing Landscapes: Gardens As Places For Spiritual, Psychological and Physical HealingrajshreeNoch keine Bewertungen
- Introduction To HospitalsDokument15 SeitenIntroduction To Hospitalskapgarg50% (2)
- Reality Therapy: Charlene Raye C. TugadeDokument8 SeitenReality Therapy: Charlene Raye C. TugadeCharlene Raye TugadeNoch keine Bewertungen
- ETHICAL ISSUES IN COUNSELING - SaidaDokument17 SeitenETHICAL ISSUES IN COUNSELING - Saidasaidahsalim67% (3)
- Essm Newsletter: Highlights From The EditionDokument24 SeitenEssm Newsletter: Highlights From The EditionRazvan BardanNoch keine Bewertungen
- Causes & Consequences of Drug AbuseDokument8 SeitenCauses & Consequences of Drug AbuseamanbioqNoch keine Bewertungen
- CEA DapagliflozinDokument11 SeitenCEA DapagliflozinAe Navarut KongsalaNoch keine Bewertungen
- AcetaminophenDokument2 SeitenAcetaminophendrugcardref100% (1)
- Vidangathanduladi Choornam YogamruthamDokument5 SeitenVidangathanduladi Choornam YogamruthamRahul KirkNoch keine Bewertungen
- Cognitive-Behavioral Therapy For Adult ADHD - An Integrative Psychosocial and Medical Approach (PDFDrive) PDFDokument253 SeitenCognitive-Behavioral Therapy For Adult ADHD - An Integrative Psychosocial and Medical Approach (PDFDrive) PDFRaúl BonillaNoch keine Bewertungen
- Mayjune 07 WebDokument40 SeitenMayjune 07 WebDave100% (2)
- Practice Test 5Dokument4 SeitenPractice Test 5Dương Lê QuýNoch keine Bewertungen
- Psychoanalytic EssayDokument7 SeitenPsychoanalytic Essayapi-462360394Noch keine Bewertungen
- UT Trauma HandbookDokument49 SeitenUT Trauma Handbooksgod34Noch keine Bewertungen
- Caries Predication, Risk Assessment and Treatment PlanningDokument74 SeitenCaries Predication, Risk Assessment and Treatment PlanningmohammadNoch keine Bewertungen
- Psych Turner SyndromeDokument13 SeitenPsych Turner SyndromeJerson CadigalNoch keine Bewertungen
- How To Grow Medicinal MarijuanaDokument9 SeitenHow To Grow Medicinal MarijuanaRoy HarperNoch keine Bewertungen
- Traumatic Brain Injury and Cerebral ResuscitationDokument56 SeitenTraumatic Brain Injury and Cerebral ResuscitationsyahirNoch keine Bewertungen
- Intake AssessmentDokument2 SeitenIntake Assessmentyourzxtruly0% (1)
- A Seminar Report On "Attitude": Seth Jai Parkash Mukand Lal Institute of Engineering and Technology, Radaur (Yamunanagar)Dokument20 SeitenA Seminar Report On "Attitude": Seth Jai Parkash Mukand Lal Institute of Engineering and Technology, Radaur (Yamunanagar)BamanNoch keine Bewertungen
- Proptosis UnilateralDokument5 SeitenProptosis UnilateralCarlos NiveloNoch keine Bewertungen
- Catholic Teaching on Gender Dysphoria and TreatmentDokument23 SeitenCatholic Teaching on Gender Dysphoria and TreatmentAntónio AlvimNoch keine Bewertungen
- Risk Management in PVDokument40 SeitenRisk Management in PVSutirtho Mukherji100% (1)
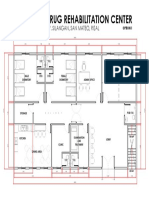
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalDokument1 SeiteProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonNoch keine Bewertungen
- Formulation, Development, and Evaluation of Indomethacin Emulgel Using Pregelatinized Starch From Ipomoea Batata TubersDokument8 SeitenFormulation, Development, and Evaluation of Indomethacin Emulgel Using Pregelatinized Starch From Ipomoea Batata Tubersaleaxndra soldanescuNoch keine Bewertungen
- Standards For Accreditation of CLINICS Practicing Modern System of Medicine (Allopathy)Dokument80 SeitenStandards For Accreditation of CLINICS Practicing Modern System of Medicine (Allopathy)shubham solankiNoch keine Bewertungen
- Drug StudyDokument4 SeitenDrug Studymisstheatricality130Noch keine Bewertungen
- Balcheva 2009, Alopecia Areata of Dental OriginDokument2 SeitenBalcheva 2009, Alopecia Areata of Dental OriginLorenzo AcerraNoch keine Bewertungen