Das könnte Ihnen auch gefallen
- Shoulder DystociaDokument20 SeitenShoulder DystociaFaridahMaksumNoch keine Bewertungen
- Shoulder DystociaDokument42 SeitenShoulder DystociaBeulah PesaramelliNoch keine Bewertungen
- Shoulder DystociaDokument7 SeitenShoulder DystociaYwagar YwagarNoch keine Bewertungen
- DystociaDokument31 SeitenDystociamarsan120% (1)
- Shoulder Dystocia ModuleDokument18 SeitenShoulder Dystocia Moduleapi-219741636100% (1)
- Umbilical Cord ProlapseDokument26 SeitenUmbilical Cord Prolapsesulekhaanoob100% (2)
- Uterine RuptureDokument21 SeitenUterine RuptureSirisha Pemma100% (7)
- Cephalopelvic DisproportionDokument6 SeitenCephalopelvic DisproportionBaljinder kaurNoch keine Bewertungen
- Cephalopelvic Disproportion (CPD)Dokument20 SeitenCephalopelvic Disproportion (CPD)Natukunda Dianah100% (4)
- Antepartum HemorrhageDokument48 SeitenAntepartum HemorrhageJoshua EvansNoch keine Bewertungen
- 35 - Retained PlacentaDokument11 Seiten35 - Retained Placentadr_asalehNoch keine Bewertungen
- Obstetric Emergencies: Shoulder DystociaDokument5 SeitenObstetric Emergencies: Shoulder DystociaYuliza SofyaNoch keine Bewertungen
- Bubble HEDokument10 SeitenBubble HEcriselda desistoNoch keine Bewertungen
- Pathophysiology of Ectopic PregnancyDokument1 SeitePathophysiology of Ectopic PregnancyLiza MinonaNoch keine Bewertungen
- Fetal MalpresentationDokument13 SeitenFetal MalpresentationJhing Rodriguez Borjal75% (4)
- Incompetent CervixDokument4 SeitenIncompetent CervixCharm Arroyo100% (1)
- The PartographDokument65 SeitenThe PartographAmyAgustinNoch keine Bewertungen
- Shoulder PresentationDokument8 SeitenShoulder PresentationvincentsharonNoch keine Bewertungen
- Obstructed LabourDokument24 SeitenObstructed LabourNatukunda Dianah50% (4)
- Dysfunctional Labor DystociaDokument8 SeitenDysfunctional Labor Dystocianursereview100% (4)
- Cephalopelvic DisproportionDokument7 SeitenCephalopelvic DisproportionEli Ayase100% (1)
- Breech PresentationDokument53 SeitenBreech PresentationVijith.V.kumar100% (6)
- Mechanism of LaborDokument12 SeitenMechanism of LaborSaidatul Safarah Md HassanNoch keine Bewertungen
- Shoulder DystociaDokument22 SeitenShoulder Dystociaamulan_aNoch keine Bewertungen
- Antepartum HaemorrhageDokument57 SeitenAntepartum HaemorrhageLady350z100% (3)
- Cephalopelvic DisproportionDokument3 SeitenCephalopelvic DisproportionEli Ayase100% (4)
- Incompetent Cervix Case Analysis Subgroup 2Dokument44 SeitenIncompetent Cervix Case Analysis Subgroup 2bunso padillaNoch keine Bewertungen
- LABOR Stage III (Placental Expulsion)Dokument6 SeitenLABOR Stage III (Placental Expulsion)api-3797941Noch keine Bewertungen
- RH IncompatibilityDokument14 SeitenRH IncompatibilityMark Terence Padua AbrenicaNoch keine Bewertungen
- Cephalopelvic DisproportionDokument2 SeitenCephalopelvic DisproportionCharmaine D. Cuevo60% (5)
- Uterine RuptureDokument19 SeitenUterine RuptureAna Denise Quinajon0% (1)
- Partogram CORRECTEDDokument45 SeitenPartogram CORRECTEDjayasankariNoch keine Bewertungen
- Breech PresentationDokument40 SeitenBreech PresentationShuhada Wahab100% (3)
- Face PresentationDokument52 SeitenFace PresentationAnnapurna DangetiNoch keine Bewertungen
- Amniotic Fluid EmbolismDokument8 SeitenAmniotic Fluid EmbolismjNoch keine Bewertungen
- Obstructed LaborDokument43 SeitenObstructed LaborNyangara Rajabu0% (2)
- Postpartum HemorrhageDokument25 SeitenPostpartum HemorrhageaKmaL67% (3)
- Postpartum Haemorrhage (PPH) : Dr. Mtumweni, MDDokument29 SeitenPostpartum Haemorrhage (PPH) : Dr. Mtumweni, MDmarco luena100% (1)
- Presentation1Dokument39 SeitenPresentation1Cartan RoobleNoch keine Bewertungen
- Lecture-33 Postpartum HemorrhageDokument50 SeitenLecture-33 Postpartum HemorrhageMadhu Sudhan Pandeya100% (2)
- Abruptio PlacentaDokument13 SeitenAbruptio Placentamiss RN92% (12)
- Antepartum HaemorrhageDokument48 SeitenAntepartum HaemorrhageDuncan JacksonNoch keine Bewertungen
- Postpartum HemorrhageDokument50 SeitenPostpartum HemorrhageSamuel SutantoNoch keine Bewertungen
- Mechanism of Labour (Normal and Abnormal)Dokument27 SeitenMechanism of Labour (Normal and Abnormal)Rani100% (1)
- Inversion of Uterus: By: Namita AryaDokument29 SeitenInversion of Uterus: By: Namita Aryanamita0% (1)
- Postpartum HemorrhageDokument3 SeitenPostpartum HemorrhageClaire Canapi BattadNoch keine Bewertungen
- CPD, Dystocia, Fetal Distress OutputDokument8 SeitenCPD, Dystocia, Fetal Distress OutputJohn Dave AbranNoch keine Bewertungen
- Multiple GestationDokument22 SeitenMultiple GestationIrish Ivy VibethNoch keine Bewertungen
- Anatomy and Physiology of PlacentaDokument5 SeitenAnatomy and Physiology of PlacentaAdrianne Basa100% (1)
- Post-Partum HemorrhageDokument15 SeitenPost-Partum Hemorrhageapi-257029163Noch keine Bewertungen
- Cephalopelvic DisproportionDokument93 SeitenCephalopelvic Disproportionkyle cunanan100% (6)
- Cephalopelvic DisproportionDokument3 SeitenCephalopelvic DisproportionAira MiyaNoch keine Bewertungen
- Post Partum Hemorrhage (PPH)Dokument77 SeitenPost Partum Hemorrhage (PPH)Aparna LaxmanNoch keine Bewertungen
- BUBBLE-HE AssessmentDokument8 SeitenBUBBLE-HE AssessmentJane Bautista100% (1)
- Shoulder Shoulder Shoulder Dystocia Dystocia DystociaDokument38 SeitenShoulder Shoulder Shoulder Dystocia Dystocia DystociaJhon Cristian Hidalgo CanalesNoch keine Bewertungen
- Dr. Chisholm Shoulder Dystocia 062607Dokument51 SeitenDr. Chisholm Shoulder Dystocia 062607kusumarizky89Noch keine Bewertungen
- Shoulder DystociaDokument27 SeitenShoulder DystociaSameena ParikhNoch keine Bewertungen
- Breech & Shoulder DystociaDokument46 SeitenBreech & Shoulder DystociaTRYPHONE zabronNoch keine Bewertungen
- Shoulder Dystocia Guideline 280720Dokument10 SeitenShoulder Dystocia Guideline 280720Ahmed SamyNoch keine Bewertungen
- Shoulder Dystocia: Clinical Practice GuidelineDokument7 SeitenShoulder Dystocia: Clinical Practice GuidelineSamantha DavisNoch keine Bewertungen
- History Taking in OrthopaedicsDokument23 SeitenHistory Taking in OrthopaedicsVaibhav Krishna100% (5)
- Acute Leukaemia Presentation 1Dokument20 SeitenAcute Leukaemia Presentation 1Vaibhav KrishnaNoch keine Bewertungen
- HIV in ChildrenDokument11 SeitenHIV in ChildrenVaibhav KrishnaNoch keine Bewertungen
- Manipal College of Medical Sciences Pokhara, Nepal: Erythema MultiformeDokument56 SeitenManipal College of Medical Sciences Pokhara, Nepal: Erythema MultiformeVaibhav KrishnaNoch keine Bewertungen
- Approach To AnemiaDokument33 SeitenApproach To AnemiaVaibhav KrishnaNoch keine Bewertungen
- Abdominal Pain in ChildrenDokument15 SeitenAbdominal Pain in ChildrenVaibhav KrishnaNoch keine Bewertungen
- Kernicterus: Sahisnuta BasnetDokument10 SeitenKernicterus: Sahisnuta BasnetVaibhav KrishnaNoch keine Bewertungen
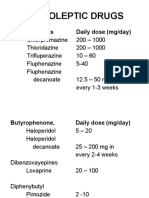
- Neuroleptic Drugs: Phenothiazines Daily Dose (Mg/day)Dokument11 SeitenNeuroleptic Drugs: Phenothiazines Daily Dose (Mg/day)Vaibhav KrishnaNoch keine Bewertungen
- Schizophrenia: Disturbances Thinking in Feeling BehaviorDokument26 SeitenSchizophrenia: Disturbances Thinking in Feeling BehaviorVaibhav KrishnaNoch keine Bewertungen
- VSDDokument29 SeitenVSDVaibhav Krishna100% (2)
- Thyroid StormDokument33 SeitenThyroid StormVaibhav Krishna50% (2)
- Neonatal JaundiceDokument33 SeitenNeonatal JaundiceVaibhav Krishna100% (2)
- Dissociation DisorderDokument33 SeitenDissociation DisorderVaibhav KrishnaNoch keine Bewertungen
- Anxiety DisorderDokument26 SeitenAnxiety DisorderVaibhav KrishnaNoch keine Bewertungen
- Antidepressants: I. Cyclic AntidepressantDokument17 SeitenAntidepressants: I. Cyclic AntidepressantVaibhav KrishnaNoch keine Bewertungen
- 3rd Stage of LabourDokument16 Seiten3rd Stage of LabourVaibhav KrishnaNoch keine Bewertungen
- Daftar Pustaka 7689Dokument20 SeitenDaftar Pustaka 7689Rivani KurniawanNoch keine Bewertungen
- Muzakarah Jawatankuasa Fatwa Majlis Kebangsaan Bagi Hal Ehwal Ugama Islam Malaysia Kali KeDokument7 SeitenMuzakarah Jawatankuasa Fatwa Majlis Kebangsaan Bagi Hal Ehwal Ugama Islam Malaysia Kali KeSiti Zubaidah ZulkhairieNoch keine Bewertungen
- Academic Calendar 2019-20 Odd Semester PDFDokument1 SeiteAcademic Calendar 2019-20 Odd Semester PDFPiyush ManwaniNoch keine Bewertungen
- Section D Textual QuestionsDokument52 SeitenSection D Textual Questionsxander ganderNoch keine Bewertungen
- Chapter 4 - Transfer FunctionsDokument36 SeitenChapter 4 - Transfer FunctionsFakhrulShahrilEzanie100% (1)
- Bhagavad Gita Ch.1 Shlok 4++Dokument1 SeiteBhagavad Gita Ch.1 Shlok 4++goldenlion1Noch keine Bewertungen
- DaybreaksDokument14 SeitenDaybreaksKYLE FRANCIS EVANoch keine Bewertungen
- Ujt and PutDokument35 SeitenUjt and Putisraeljumbo100% (1)
- CA IPCC Accounting Guideline Answers May 2015Dokument24 SeitenCA IPCC Accounting Guideline Answers May 2015Prashant PandeyNoch keine Bewertungen
- The Challenge of Drug Discovery in The 21st CenturyDokument5 SeitenThe Challenge of Drug Discovery in The 21st CenturyHugo de CeaNoch keine Bewertungen
- "The Grace Period Has Ended": An Approach To Operationalize GDPR RequirementsDokument11 Seiten"The Grace Period Has Ended": An Approach To Operationalize GDPR RequirementsDriff SedikNoch keine Bewertungen
- TARA FrameworkDokument2 SeitenTARA Frameworkdominic100% (1)
- MAT 120 NSU SyllabusDokument5 SeitenMAT 120 NSU SyllabusChowdhury_Irad_2937100% (1)
- Group 4 CariCRIS Case SubmissionDokument6 SeitenGroup 4 CariCRIS Case SubmissionKingsuk MaityNoch keine Bewertungen
- NotesDokument2 SeitenNotesNoella Marie BaronNoch keine Bewertungen
- Docshare - Tips Upstream Advanced c1 Test BookletDokument3 SeitenDocshare - Tips Upstream Advanced c1 Test BookletCosmin OaieNoch keine Bewertungen
- Astro ExamDokument7 SeitenAstro ExamRitu DuaNoch keine Bewertungen
- The University of Southern Mindanao VisionDokument9 SeitenThe University of Southern Mindanao VisionNorhainie GuimbalananNoch keine Bewertungen
- SF3300Dokument2 SeitenSF3300benoitNoch keine Bewertungen
- Bottoms y Sparks - Legitimacy - and - Imprisonment - Revisited PDFDokument29 SeitenBottoms y Sparks - Legitimacy - and - Imprisonment - Revisited PDFrossana gaunaNoch keine Bewertungen
- Javier Guzman v. City of Cranston, 812 F.2d 24, 1st Cir. (1987)Dokument4 SeitenJavier Guzman v. City of Cranston, 812 F.2d 24, 1st Cir. (1987)Scribd Government DocsNoch keine Bewertungen
- Concept Paper For Business ResearchDokument4 SeitenConcept Paper For Business ResearchRobertchristian RagaNoch keine Bewertungen
- Thousand 6, One Thousand 7, One Thousand 8, One Thousand 9, One Thousand 10Dokument7 SeitenThousand 6, One Thousand 7, One Thousand 8, One Thousand 9, One Thousand 10Nhazie NyzeNoch keine Bewertungen
- Design of Irrigation CanalsDokument6 SeitenDesign of Irrigation CanalsSaad ShauketNoch keine Bewertungen
- AZ-300 - Azure Solutions Architect TechnologiesDokument3 SeitenAZ-300 - Azure Solutions Architect TechnologiesAmar Singh100% (1)
- Revised Market Making Agreement 31.03Dokument13 SeitenRevised Market Making Agreement 31.03Bhavin SagarNoch keine Bewertungen
- Cranial Deformity in The Pueblo AreaDokument3 SeitenCranial Deformity in The Pueblo AreaSlavica JovanovicNoch keine Bewertungen
- Στέργος Νεκτάριος-Μικκιος-CVDokument4 SeitenΣτέργος Νεκτάριος-Μικκιος-CVNektarios MikkiosNoch keine Bewertungen
- I. Revised Penal Code (RPC) and Related Special Laws: Riminal AWDokument11 SeitenI. Revised Penal Code (RPC) and Related Special Laws: Riminal AWMc Vharn CatreNoch keine Bewertungen
- HDLSS Numerical Assignments - DOC FormatDokument3 SeitenHDLSS Numerical Assignments - DOC FormatNikhil UpadhyayNoch keine Bewertungen