Das könnte Ihnen auch gefallen
- Neonatal Jaundice CmeDokument39 SeitenNeonatal Jaundice CmeGideon K. Mutai100% (1)
- Neonatal Jaundice (Wong)Dokument54 SeitenNeonatal Jaundice (Wong)Siti Hajar100% (1)
- Neonatal Jaundice Lecture,,By DR Kassahun GirmaDokument25 SeitenNeonatal Jaundice Lecture,,By DR Kassahun GirmaKassahun Girma GelawNoch keine Bewertungen
- Neonatal Jaundice CME ANisDokument47 SeitenNeonatal Jaundice CME ANisAnisNoch keine Bewertungen
- JaundiceDokument41 SeitenJaundicesavina hasbianiNoch keine Bewertungen
- Neo JaundiceDokument67 SeitenNeo Jaundicemanisha thakur100% (1)
- Neonatal JaundiceDokument48 SeitenNeonatal Jaundicelordoftheweb100% (22)
- OligohydramniosDokument4 SeitenOligohydramniossalamredNoch keine Bewertungen
- Ectopic PregnancyDokument26 SeitenEctopic PregnancysandhyakrishnanNoch keine Bewertungen
- Approach To Neonatal JaundiceDokument73 SeitenApproach To Neonatal JaundiceG Venkatesh50% (2)
- Neonatal HyperbilirubinemiaDokument36 SeitenNeonatal HyperbilirubinemiamahmmoudeltaweelNoch keine Bewertungen
- Meconium Aspiration Syndrome (MAS)Dokument12 SeitenMeconium Aspiration Syndrome (MAS)Angela AmaoNoch keine Bewertungen
- HyperbilirubinemiaDokument10 SeitenHyperbilirubinemiachiboogs456100% (1)
- CPDDokument14 SeitenCPDmaezuNoch keine Bewertungen
- Neonatal HypoglycemiaDokument22 SeitenNeonatal HypoglycemiaRonak Sheth100% (3)
- ABO Incompatibility: By: Marvi Mae Jimena Rosean Marvi Joy M. YunsayDokument14 SeitenABO Incompatibility: By: Marvi Mae Jimena Rosean Marvi Joy M. Yunsaysagameteiro100% (1)
- Asphyxia NeonatorumDokument34 SeitenAsphyxia NeonatorumListya Paramita100% (1)
- Congenital Diaphragmatic HerniaDokument21 SeitenCongenital Diaphragmatic HerniaJennifer Dixon100% (1)
- HyperbilirubinemiaDokument29 SeitenHyperbilirubinemiaCham Ingalla Pascion88% (8)
- Hypertension in Pregnancy: Margaret S. Hamilton, DNS, RNDokument33 SeitenHypertension in Pregnancy: Margaret S. Hamilton, DNS, RNHaji RajiNoch keine Bewertungen
- Neonatal Jaundice DrkumarDokument44 SeitenNeonatal Jaundice Drkumarvasu_5iveNoch keine Bewertungen
- OB GDM CasepresDokument102 SeitenOB GDM Casepreskitten garciaNoch keine Bewertungen
- Neonatal Jaundice: Dr. Nahed Al-NaggerDokument25 SeitenNeonatal Jaundice: Dr. Nahed Al-NaggerElok Pratiwi100% (2)
- Post-Partum HemorrhageDokument15 SeitenPost-Partum Hemorrhageapi-257029163Noch keine Bewertungen
- Jaundice-Neonatal 2016Dokument45 SeitenJaundice-Neonatal 2016Awatef AbushhiwaNoch keine Bewertungen
- Torch InfectionsDokument27 SeitenTorch InfectionsSimi SaiPrasoonNoch keine Bewertungen
- Abhay Jain Roll No 126Dokument20 SeitenAbhay Jain Roll No 126abhay jainNoch keine Bewertungen
- Ophthalmia NeonatorumDokument19 SeitenOphthalmia NeonatorumSanthu Tvm100% (1)
- Hyperbilirubinemia Case PresentationDokument25 SeitenHyperbilirubinemia Case PresentationEricka B. Banaszczuk100% (3)
- Perinatal Asphyxia - Outline of Pathophysiology and Recent Trends in ManagementDokument31 SeitenPerinatal Asphyxia - Outline of Pathophysiology and Recent Trends in Managementokwadha simionNoch keine Bewertungen
- Neonatal Hyperbilirubinemia and JaundiceDokument8 SeitenNeonatal Hyperbilirubinemia and JaundiceAndreea GeorgianaNoch keine Bewertungen
- HIV in PregnancyDokument28 SeitenHIV in PregnancyRaja100% (1)
- Intrauterine Growth Restriction (IUGR)Dokument7 SeitenIntrauterine Growth Restriction (IUGR)redhoprayuda100% (1)
- Anemia in PregnancyDokument17 SeitenAnemia in Pregnancytharmasilen100% (1)
- High Risk NewbornDokument21 SeitenHigh Risk Newbornnaga maniNoch keine Bewertungen
- Care of Neonate With HyperbilirubinemiaDokument11 SeitenCare of Neonate With HyperbilirubinemiaKakali ChakrabortyNoch keine Bewertungen
- Congenital SyphilisDokument6 SeitenCongenital SyphilisFrozen Pandora MahayaNoch keine Bewertungen
- Neonatal Hyperglycemia1Dokument17 SeitenNeonatal Hyperglycemia1Abhinav Mitra VatsNoch keine Bewertungen
- Cord Presentation and ProlapseDokument4 SeitenCord Presentation and ProlapseAnnapurna Dangeti100% (2)
- Breech PresentationDokument85 SeitenBreech Presentationwidya vannesaNoch keine Bewertungen
- Nursing Care of HyperbilirubinemiaDokument12 SeitenNursing Care of HyperbilirubinemiaFri-fri Manila67% (3)
- Meconium Aspiration SyndromeDokument29 SeitenMeconium Aspiration SyndromeAlwin Varghese T0% (1)
- Neonatal HyperbilirubinemiaDokument22 SeitenNeonatal Hyperbilirubinemiajoza29Noch keine Bewertungen
- Harika Priyanka. K Asst. Professor AconDokument30 SeitenHarika Priyanka. K Asst. Professor AconArchana MoreyNoch keine Bewertungen
- GDMDokument16 SeitenGDMNorshahidah IedaNoch keine Bewertungen
- Baby at Risk (NBU) NotesDokument131 SeitenBaby at Risk (NBU) NotesMercy KeruboNoch keine Bewertungen
- Management of Neonatal JaundiceDokument22 SeitenManagement of Neonatal JaundiceSuhazeli Abdullah100% (1)
- Case Study On Meninomyocele (Repaired) PDokument29 SeitenCase Study On Meninomyocele (Repaired) Pcharanjit kaur100% (1)
- Neonatal JaundiceDokument3 SeitenNeonatal JaundicevorezNoch keine Bewertungen
- Multiple PregnancyDokument20 SeitenMultiple PregnancyNurul Fahmiza TumiranNoch keine Bewertungen
- Anorectal MalformationDokument28 SeitenAnorectal MalformationJaya Prabha33% (3)
- 27 Purpureal Venous Thrombosis and Pulmonary Embolism by Shambuling HebballiDokument14 Seiten27 Purpureal Venous Thrombosis and Pulmonary Embolism by Shambuling HebballiSamhitha Ayurvedic ChennaiNoch keine Bewertungen
- Breech PresentationDokument40 SeitenBreech PresentationShuhada Wahab100% (3)
- Newborn AssessmentDokument9 SeitenNewborn Assessmentapi-237668254Noch keine Bewertungen
- Placenta Previa (New) - 1Dokument32 SeitenPlacenta Previa (New) - 1Ibrahim ZainabNoch keine Bewertungen
- Primary Uterine InertiaDokument4 SeitenPrimary Uterine InertiaTrisha Cayabyab100% (1)
- Hemolytic Disease of The NewbornDokument43 SeitenHemolytic Disease of The Newbornalibayaty1Noch keine Bewertungen
- Icterus NeonatarumDokument64 SeitenIcterus NeonatarumDeepti KukretiNoch keine Bewertungen
- Neonatal JaundiceDokument45 SeitenNeonatal JaundiceDrhassan HuseinNoch keine Bewertungen
- Approach To Neonatal HyperbilirubinemiaDokument34 SeitenApproach To Neonatal HyperbilirubinemiaNilesh HatzadeNoch keine Bewertungen
- History Taking in OrthopaedicsDokument23 SeitenHistory Taking in OrthopaedicsVaibhav Krishna100% (5)
- Acute Leukaemia Presentation 1Dokument20 SeitenAcute Leukaemia Presentation 1Vaibhav KrishnaNoch keine Bewertungen
- Manipal College of Medical Sciences Pokhara, Nepal: Erythema MultiformeDokument56 SeitenManipal College of Medical Sciences Pokhara, Nepal: Erythema MultiformeVaibhav KrishnaNoch keine Bewertungen
- Approach To AnemiaDokument33 SeitenApproach To AnemiaVaibhav KrishnaNoch keine Bewertungen
- HIV in ChildrenDokument11 SeitenHIV in ChildrenVaibhav KrishnaNoch keine Bewertungen
- Kernicterus: Sahisnuta BasnetDokument10 SeitenKernicterus: Sahisnuta BasnetVaibhav KrishnaNoch keine Bewertungen
- Abdominal Pain in ChildrenDokument15 SeitenAbdominal Pain in ChildrenVaibhav KrishnaNoch keine Bewertungen
- Schizophrenia: Disturbances Thinking in Feeling BehaviorDokument26 SeitenSchizophrenia: Disturbances Thinking in Feeling BehaviorVaibhav KrishnaNoch keine Bewertungen
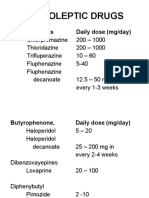
- Neuroleptic Drugs: Phenothiazines Daily Dose (Mg/day)Dokument11 SeitenNeuroleptic Drugs: Phenothiazines Daily Dose (Mg/day)Vaibhav KrishnaNoch keine Bewertungen
- VSDDokument29 SeitenVSDVaibhav Krishna100% (2)
- Antidepressants: I. Cyclic AntidepressantDokument17 SeitenAntidepressants: I. Cyclic AntidepressantVaibhav KrishnaNoch keine Bewertungen
- Dissociation DisorderDokument33 SeitenDissociation DisorderVaibhav KrishnaNoch keine Bewertungen
- 3rd Stage of LabourDokument16 Seiten3rd Stage of LabourVaibhav KrishnaNoch keine Bewertungen
- Shoulder DystociaDokument38 SeitenShoulder DystociaVaibhav Krishna100% (1)
- Anxiety DisorderDokument26 SeitenAnxiety DisorderVaibhav KrishnaNoch keine Bewertungen
- Thyroid StormDokument33 SeitenThyroid StormVaibhav Krishna50% (2)
- Intellectual Disabilities ScriptDokument6 SeitenIntellectual Disabilities Scriptapi-302509341Noch keine Bewertungen
- 1) Introduction To Microbiology - HistoryDokument37 Seiten1) Introduction To Microbiology - HistoryJustin Dave ManantanNoch keine Bewertungen
- Report 1 - History of Medical TechnologyDokument1 SeiteReport 1 - History of Medical TechnologyMaxine TaeyeonNoch keine Bewertungen
- Set A: Community Health Nursing and Care of Mother and ChildDokument11 SeitenSet A: Community Health Nursing and Care of Mother and ChildAldrin NavarroNoch keine Bewertungen
- Life Expectancy Powerpoint PresentationDokument6 SeitenLife Expectancy Powerpoint PresentationAlejandro MendozaNoch keine Bewertungen
- Step by Step Interventional Ultrasound in Obstetrics and GynaecologyDokument116 SeitenStep by Step Interventional Ultrasound in Obstetrics and GynaecologySahal Beli100% (1)
- BPC-157 - Scientific Review On Usage, Dosage, Side Effects - ExamineDokument10 SeitenBPC-157 - Scientific Review On Usage, Dosage, Side Effects - Examineozman blooriNoch keine Bewertungen
- The Science of Sleep: A Brief Guide On How To Sleep Better Every NightDokument2 SeitenThe Science of Sleep: A Brief Guide On How To Sleep Better Every NightMark Anthony RaymundoNoch keine Bewertungen
- Bearing Habits and Garden Practices To Induce FruitfulnessDokument6 SeitenBearing Habits and Garden Practices To Induce FruitfulnessHEGDErv1964Noch keine Bewertungen
- Mark Kilimek AUDIO NOTESDokument6 SeitenMark Kilimek AUDIO NOTESHannah Perkins100% (2)
- 1010 Research Paper 1Dokument10 Seiten1010 Research Paper 1api-442331287Noch keine Bewertungen
- ДСТУ EN ISO 13408-2 2019Dokument50 SeitenДСТУ EN ISO 13408-2 2019DenisNoch keine Bewertungen
- 978-615-5169-15-1 Physiology Anatomy PDFDokument236 Seiten978-615-5169-15-1 Physiology Anatomy PDFSuresh Kanna0% (1)
- Biochemical Changes During PregnancyDokument15 SeitenBiochemical Changes During Pregnancyz100% (1)
- PCORI Methodology Standards Curriculum Research Questions 3Dokument13 SeitenPCORI Methodology Standards Curriculum Research Questions 3Krizele Acu PagalananNoch keine Bewertungen
- Atkins EnzimasDokument5 SeitenAtkins EnzimasConstanza Espinoza LaraNoch keine Bewertungen
- Blood Sugar Insulin Polyuria Polydipsia PolyphagiaDokument7 SeitenBlood Sugar Insulin Polyuria Polydipsia PolyphagiankirrNoch keine Bewertungen
- Effect of Organic Manure On Growth and Yield of Strawberry: January 2014Dokument5 SeitenEffect of Organic Manure On Growth and Yield of Strawberry: January 2014LekhonVlogsNoch keine Bewertungen
- Water, Sanitation and Hygiene Manual: WASH Training For Hygiene Promotion StaffDokument20 SeitenWater, Sanitation and Hygiene Manual: WASH Training For Hygiene Promotion StaffSadashiv RahaneNoch keine Bewertungen
- Medical Language 3rd Edition Test Bank Susan M TurleyDokument37 SeitenMedical Language 3rd Edition Test Bank Susan M Turleykatieterryrlrb100% (12)
- Sr. No. Cghs Treatment Procedure/Investigation List Non-NABH/Non - NABL Rates Nabh/Nabl RatesDokument49 SeitenSr. No. Cghs Treatment Procedure/Investigation List Non-NABH/Non - NABL Rates Nabh/Nabl RatesADDECC INFO INDIANoch keine Bewertungen
- Speaking Part 3 Update 2022Dokument7 SeitenSpeaking Part 3 Update 2022Nhi LêNoch keine Bewertungen
- Chemical Safety TrainingDokument229 SeitenChemical Safety TrainingOmprakaash MokideNoch keine Bewertungen
- SP 32434 Warm Up and Cool Down - Indd PDFDokument1 SeiteSP 32434 Warm Up and Cool Down - Indd PDFMylene EntionNoch keine Bewertungen
- Family Planning (Teaching Plan) Ana AlcasabasDokument6 SeitenFamily Planning (Teaching Plan) Ana Alcasabasiammerbinpransisko75% (4)
- CBSE Class 7 Science MCQs-Respiration in OrganismsDokument2 SeitenCBSE Class 7 Science MCQs-Respiration in Organismssiba padhy100% (3)
- RCDSO Guidelines Implant Dentistry PDFDokument16 SeitenRCDSO Guidelines Implant Dentistry PDFl4j0b9Noch keine Bewertungen
- HomeostasisDokument2 SeitenHomeostasisAnn Calindo EstafiaNoch keine Bewertungen
- Benign Odontogenic Tumors of Jaws (AmeloblastomaDokument70 SeitenBenign Odontogenic Tumors of Jaws (Ameloblastomagalina poberezhnikNoch keine Bewertungen
- Epidemiology of Knee Injuries Among Boys and Girls in US High School AthleticsDokument7 SeitenEpidemiology of Knee Injuries Among Boys and Girls in US High School AthleticsbomgorilaoNoch keine Bewertungen