Das könnte Ihnen auch gefallen
- 6th Central Pay Commission Salary CalculatorDokument15 Seiten6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDokument15 Seiten6th Central Pay Commission Salary Calculatorrakhonde100% (436)
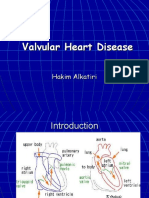
- Valvular Heart DiseaseDokument85 SeitenValvular Heart DiseaseWilliam Lie100% (2)
- Essential Facts in Cardiovascular Medicine: Board Review and Clinical PearlsVon EverandEssential Facts in Cardiovascular Medicine: Board Review and Clinical PearlsNoch keine Bewertungen
- Valvular Heart DiseaseDokument10 SeitenValvular Heart DiseaseEzyan SyaminNoch keine Bewertungen
- Valvular Heart Disease and Non Cardiac Surgery: Lakshmi P. YalavarthyDokument44 SeitenValvular Heart Disease and Non Cardiac Surgery: Lakshmi P. YalavarthyLakshmi YalavarthyNoch keine Bewertungen
- Questions Related To CodesDokument10 SeitenQuestions Related To CodesMayur Mandrekar100% (1)
- Wk7 PLP Cardiovascular Disorder Part 1,2,3,4Dokument210 SeitenWk7 PLP Cardiovascular Disorder Part 1,2,3,4claire yowsNoch keine Bewertungen
- Valvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMDokument69 SeitenValvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMAbanoub AwadallaNoch keine Bewertungen
- Peds Shelf NotesDokument74 SeitenPeds Shelf NotesRandy BornmannNoch keine Bewertungen
- Non-Cyanotic Congenital Heart Disease-UpDate 4-22-53Dokument136 SeitenNon-Cyanotic Congenital Heart Disease-UpDate 4-22-53getnusNoch keine Bewertungen
- WhatsApp Chat With Chinnu HeartDokument30 SeitenWhatsApp Chat With Chinnu HeartSäi DäťťaNoch keine Bewertungen
- Aortic RegurgitationDokument41 SeitenAortic RegurgitationMedi PutraNoch keine Bewertungen
- Achd Ug OriginalDokument43 SeitenAchd Ug OriginalchristyNoch keine Bewertungen
- Mitral StenosisDokument17 SeitenMitral StenosisMuhammad Alauddin Sarwar100% (8)
- A Handbook of Multivalvular and Prosthetic Valve DiseaseVon EverandA Handbook of Multivalvular and Prosthetic Valve DiseaseNoch keine Bewertungen
- UMS20 Medical 20 Short 20 and 20 Long 20 Cases 20 Record 20 Second 20 EditiDokument132 SeitenUMS20 Medical 20 Short 20 and 20 Long 20 Cases 20 Record 20 Second 20 EditiUchiha AnzarNoch keine Bewertungen
- Jansenkoh MRCP PacesDokument209 SeitenJansenkoh MRCP PacesBob Yong83% (6)
- Pregnancy With MS MRDokument74 SeitenPregnancy With MS MRRaj K SharmaNoch keine Bewertungen
- Valvular Heart DiseaseDokument27 SeitenValvular Heart DiseaseOwen J. WieseNoch keine Bewertungen
- Farmall 105u115u 16x16transDokument2.233 SeitenFarmall 105u115u 16x16transchrideerNoch keine Bewertungen
- wk8 Nursing Care of A Family When A Child Has An Immune Disorders Part 2Dokument32 Seitenwk8 Nursing Care of A Family When A Child Has An Immune Disorders Part 2claire yowsNoch keine Bewertungen
- Aortic StenosisDokument37 SeitenAortic Stenosissarguss14Noch keine Bewertungen
- LeasingDokument18 SeitenLeasingsunithakravi0% (1)
- Mitral StenosisDokument48 SeitenMitral StenosiskornbergwiNoch keine Bewertungen
- Bergey's Manual of Systematic Bacteriology and Determinative BacteriologyDokument2 SeitenBergey's Manual of Systematic Bacteriology and Determinative BacteriologyGeetha Anjali0% (1)
- Strip Seal Expansion JointDokument13 SeitenStrip Seal Expansion JointsmithNoch keine Bewertungen
- Master Handover Rev 4-2013Dokument8 SeitenMaster Handover Rev 4-2013MeysamGholizadehNoch keine Bewertungen
- I. Leadership/ Potential and Accomplishments Criteria A. InnovationsDokument5 SeitenI. Leadership/ Potential and Accomplishments Criteria A. InnovationsDEXTER LLOYD CATIAG100% (1)
- Valvular 2005Dokument32 SeitenValvular 2005rajeeNoch keine Bewertungen
- Penyakit KatupDokument31 SeitenPenyakit KatupAdinda Suci MaghfiraNoch keine Bewertungen
- MS MR As ArDokument21 SeitenMS MR As ArTamim IshtiaqueNoch keine Bewertungen
- VHD Inter FinalDokument84 SeitenVHD Inter Finalfitrah fajrianiNoch keine Bewertungen
- Cvs-k7-Valvular Heart Disease Nora2010Dokument52 SeitenCvs-k7-Valvular Heart Disease Nora2010shiloinNoch keine Bewertungen
- Valvular Heart Disease: Hakim AlkatiriDokument84 SeitenValvular Heart Disease: Hakim AlkatiriFNoch keine Bewertungen
- Mitral Stenosis: JONES Criteria - 2015 Modification Major CriteriaDokument13 SeitenMitral Stenosis: JONES Criteria - 2015 Modification Major CriteriaBiswarup PurkayasthaNoch keine Bewertungen
- Valvular UpdateDokument44 SeitenValvular UpdateUlmi FadillahNoch keine Bewertungen
- Duct Dependent Lesions - PPSXDokument41 SeitenDuct Dependent Lesions - PPSXSindujaNoch keine Bewertungen
- Regurgitant Lesion - My SeminarDokument121 SeitenRegurgitant Lesion - My SeminarAbnet WondimuNoch keine Bewertungen
- Penyakit Katup Jantung: Dr. Tjatur Winarsanto SPPD Rs CiremaiDokument59 SeitenPenyakit Katup Jantung: Dr. Tjatur Winarsanto SPPD Rs CiremaianisamayaNoch keine Bewertungen
- Mitral Regurgitation Etiology and Pathophysiology: Physical ExaminationsDokument11 SeitenMitral Regurgitation Etiology and Pathophysiology: Physical ExaminationsDelmy SanjayaNoch keine Bewertungen
- Valvular Heart Disease: Bekele T. (MD)Dokument47 SeitenValvular Heart Disease: Bekele T. (MD)alehegn beleteNoch keine Bewertungen
- 7 PENYAKIT JANTUNG BAWAAN DR - YusraDokument57 Seiten7 PENYAKIT JANTUNG BAWAAN DR - YusraSurya ArhNoch keine Bewertungen
- Classification of Cardiac Malformations: Daniel Bernstein's (Clinical + Physiopathological)Dokument28 SeitenClassification of Cardiac Malformations: Daniel Bernstein's (Clinical + Physiopathological)Sandyka AleNoch keine Bewertungen
- Pathophys VHD-Final (Budi S. Pikir)Dokument155 SeitenPathophys VHD-Final (Budi S. Pikir)Muhammad DaviqNoch keine Bewertungen
- Valvular DiseasesDokument45 SeitenValvular DiseasesKen WayNoch keine Bewertungen
- Valvular Heart Disease and The Cardiac ExamDokument42 SeitenValvular Heart Disease and The Cardiac ExamJuwanto WakiminNoch keine Bewertungen
- Mitral StenosisDokument95 SeitenMitral StenosisAbnet WondimuNoch keine Bewertungen
- VSD 180207074930Dokument33 SeitenVSD 180207074930widyaNoch keine Bewertungen
- Ilmu Dan Seni Pengabilan KeputusanDokument17 SeitenIlmu Dan Seni Pengabilan KeputusanMuhammad Khoirul SodiqNoch keine Bewertungen
- 2 Valvular Heart Disease1Dokument87 Seiten2 Valvular Heart Disease1Danny DesuNoch keine Bewertungen
- Mitral StenosisDokument37 SeitenMitral StenosisInsan IlmanNoch keine Bewertungen
- Pleno Minggu 3 Blok 3.2Dokument57 SeitenPleno Minggu 3 Blok 3.2ima_nekonayagiNoch keine Bewertungen
- Mitral Sihar Presentasi PJTDokument69 SeitenMitral Sihar Presentasi PJTJaclinNoch keine Bewertungen
- Valvular Heart Disease and The Cardiac Exam: Charlotte Bai, M.D. Internal Medicine Board Review May 28, 2009Dokument42 SeitenValvular Heart Disease and The Cardiac Exam: Charlotte Bai, M.D. Internal Medicine Board Review May 28, 2009Ami DhaniaNoch keine Bewertungen
- Lecture 17a VHDDokument70 SeitenLecture 17a VHDKishan ArrumugamNoch keine Bewertungen
- Valvular Heart Disease IM 8-12 NewDokument80 SeitenValvular Heart Disease IM 8-12 NewRachilla Arandita SaraswatiNoch keine Bewertungen
- Falla Ventriculo DerechoDokument6 SeitenFalla Ventriculo DerechoMartin M.V.Noch keine Bewertungen
- Valvular Heart DiseasesDokument86 SeitenValvular Heart DiseasesParvathy R NairNoch keine Bewertungen
- Aortic Stenosis - LecturioDokument13 SeitenAortic Stenosis - Lecturiokujtimepira2Noch keine Bewertungen
- 4.17 Keane Aortic StenosisDokument61 Seiten4.17 Keane Aortic StenosisFarman JaaferNoch keine Bewertungen
- Mitral Stenosis-RarestDokument9 SeitenMitral Stenosis-RarestWen Jie LauNoch keine Bewertungen
- Curs de Chirurgie Cardiaca PT StudentiDokument86 SeitenCurs de Chirurgie Cardiaca PT StudentiLozan GabrielaNoch keine Bewertungen
- Mitral Stenosis, NicvdDokument33 SeitenMitral Stenosis, NicvdNavojit ChowdhuryNoch keine Bewertungen
- Mitral Valve RepairDokument109 SeitenMitral Valve RepairheldhiNoch keine Bewertungen
- 28 Valvular Heart Disease DR - YusraDokument46 Seiten28 Valvular Heart Disease DR - YusraSurya ArhNoch keine Bewertungen
- Valvular Heart Disease1Dokument80 SeitenValvular Heart Disease1Abnet WondimuNoch keine Bewertungen
- Mitral Stenosis Mitral StenosisDokument68 SeitenMitral Stenosis Mitral StenosisnijasNoch keine Bewertungen
- Acyanotic CHDDokument83 SeitenAcyanotic CHDmrinmayee deshmukhNoch keine Bewertungen
- Low Risk NFDokument26 SeitenLow Risk NFfallenczarNoch keine Bewertungen
- Shortlisting Quick Reference: Reviewing and RecommendationsDokument1 SeiteShortlisting Quick Reference: Reviewing and RecommendationsfallenczarNoch keine Bewertungen
- Cellulitis Guidelines, CREST, 05 PDFDokument31 SeitenCellulitis Guidelines, CREST, 05 PDFanathasia_christineNoch keine Bewertungen
- GCSF Policy WalesDokument7 SeitenGCSF Policy WalesfallenczarNoch keine Bewertungen
- Wild 2017Dokument7 SeitenWild 2017fallenczarNoch keine Bewertungen
- BP Control in CKD - Beyond The GuidelinesDokument15 SeitenBP Control in CKD - Beyond The GuidelinesfallenczarNoch keine Bewertungen
- Random Number GeneratorDokument2 SeitenRandom Number GeneratorfallenczarNoch keine Bewertungen
- Table: Causes of and Conditions Associated With BronchiectasisDokument6 SeitenTable: Causes of and Conditions Associated With BronchiectasisfallenczarNoch keine Bewertungen
- SalmonellaDokument26 SeitenSalmonellafallenczarNoch keine Bewertungen
- Neurology Loc II-common CasesDokument64 SeitenNeurology Loc II-common CasesfallenczarNoch keine Bewertungen
- Basic Mecahnical Ventilation - Critical Concepts - PulmonaryDokument54 SeitenBasic Mecahnical Ventilation - Critical Concepts - PulmonaryMarcela Catalina Fandiño VargasNoch keine Bewertungen
- SLR Ventilator Weaning Education PresentationDokument48 SeitenSLR Ventilator Weaning Education Presentationfallenczar100% (1)
- Examination of The AbdomenDokument2 SeitenExamination of The AbdomenfallenczarNoch keine Bewertungen
- COPD - Diagnosis and ManagementDokument12 SeitenCOPD - Diagnosis and ManagementfallenczarNoch keine Bewertungen
- Table: Causes of and Conditions Associated With BronchiectasisDokument6 SeitenTable: Causes of and Conditions Associated With BronchiectasisfallenczarNoch keine Bewertungen
- Wastewater Treatment Lab TestDokument8 SeitenWastewater Treatment Lab TesthuyNoch keine Bewertungen
- Components of FitnessDokument3 SeitenComponents of Fitnessapi-3830277100% (1)
- Techno LabDokument3 SeitenTechno LabA M FaisalNoch keine Bewertungen
- Minibeasts Differentiated Reading Comprehension ActivityDokument15 SeitenMinibeasts Differentiated Reading Comprehension Activitymariam helmyNoch keine Bewertungen
- 1.indentify The Functions of Various Keys On The Key BoardDokument83 Seiten1.indentify The Functions of Various Keys On The Key BoardMuhammad AbbasNoch keine Bewertungen
- Measurement of Poverty and Poverty of Measurement: Martin GreeleyDokument15 SeitenMeasurement of Poverty and Poverty of Measurement: Martin GreeleyKule89Noch keine Bewertungen
- Pin ContentDokument20 SeitenPin ContentSwetha100% (2)
- MahuaDokument12 SeitenMahuaVinay ChhalotreNoch keine Bewertungen
- Conditional Type 0Dokument16 SeitenConditional Type 0marore100% (1)
- Comparatives and SuperlativesDokument2 SeitenComparatives and Superlativesjcarlosgf60% (5)
- Material Science & Metallurgy: Third Semester B.E. Degree (CBCS) Examination, Dec.2016/Jan.2017Dokument2 SeitenMaterial Science & Metallurgy: Third Semester B.E. Degree (CBCS) Examination, Dec.2016/Jan.2017Shaikh MuzaffarNoch keine Bewertungen
- Am Jf211 - Jul 04Dokument4 SeitenAm Jf211 - Jul 04ilham_metallurgy6744Noch keine Bewertungen
- Manualevu VheDokument60 SeitenManualevu VheThariqNoch keine Bewertungen
- EO MNC 10 June 2022Dokument4 SeitenEO MNC 10 June 2022LeulaDianneCantosNoch keine Bewertungen
- Bcba CourseworkDokument8 SeitenBcba Courseworkafjwoamzdxwmct100% (2)
- Passive In-Line Chlorination For Drinking Water DiDokument18 SeitenPassive In-Line Chlorination For Drinking Water DitefovNoch keine Bewertungen
- Natural Resources NotesDokument5 SeitenNatural Resources NotesRajesh Kumar GuptaNoch keine Bewertungen
- Hilti AnchorsDokument202 SeitenHilti AnchorsmwendaNoch keine Bewertungen
- Important Topics RTCDokument18 SeitenImportant Topics RTCjoydeep12Noch keine Bewertungen
- 1716 ch05Dokument103 Seiten1716 ch05parisliuhotmail.comNoch keine Bewertungen
- Nutrients: Dietary Fiber, Atherosclerosis, and Cardiovascular DiseaseDokument11 SeitenNutrients: Dietary Fiber, Atherosclerosis, and Cardiovascular Diseasemichael palitNoch keine Bewertungen