Das könnte Ihnen auch gefallen
- ST Segment and T Waves:: Ischemia, Infarction, Drug & Electrolyte EffectsDokument34 SeitenST Segment and T Waves:: Ischemia, Infarction, Drug & Electrolyte EffectsHibba NasserNoch keine Bewertungen
- 4 - Intracranial TumorsDokument35 Seiten4 - Intracranial TumorsHibba NasserNoch keine Bewertungen
- Myasthenia Gravis Guest LectureDokument43 SeitenMyasthenia Gravis Guest LectureHibba NasserNoch keine Bewertungen
- Myasthenia GravisDokument55 SeitenMyasthenia GravisHibba NasserNoch keine Bewertungen
- Myasthenia Gravis: An Autoimmune Neurologic DisorderDokument16 SeitenMyasthenia Gravis: An Autoimmune Neurologic DisorderHibba NasserNoch keine Bewertungen
- Myasthenia Gravis: General Thoracic SurgeryDokument28 SeitenMyasthenia Gravis: General Thoracic SurgeryHibba NasserNoch keine Bewertungen
- Myasthenia GravisDokument15 SeitenMyasthenia GravisHibba NasserNoch keine Bewertungen
- Myasthenia GravisDokument15 SeitenMyasthenia GravisHibba NasserNoch keine Bewertungen
- Myasthenia GravisDokument15 SeitenMyasthenia GravisHibba NasserNoch keine Bewertungen
- Myasthenia GravisDokument43 SeitenMyasthenia GravisNgurah Arya PradnyantaraNoch keine Bewertungen
- Myasthenia Gravis: General Thoracic SurgeryDokument28 SeitenMyasthenia Gravis: General Thoracic SurgeryHibba NasserNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- COVID-19 Cytokine Storm Syndrome: Identification and TreatmentDokument13 SeitenCOVID-19 Cytokine Storm Syndrome: Identification and TreatmentIoana PelinNoch keine Bewertungen
- Pneumonia CaseDokument62 SeitenPneumonia CaseDyaneGepteNoch keine Bewertungen
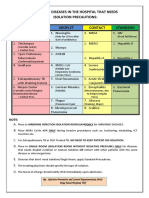
- Common Hospital Diseases Requiring Isolation PrecautionsDokument1 SeiteCommon Hospital Diseases Requiring Isolation Precautionsjerimiah_manzonNoch keine Bewertungen
- Investigate CAP Severity & CausesDokument27 SeitenInvestigate CAP Severity & CausesRoshana Mallawaarachchi0% (1)
- Manual on Nursing Health Assessment GuideDokument195 SeitenManual on Nursing Health Assessment Guidetiredandsleepy100% (5)
- Physical Examination in Respiratory SystemDokument58 SeitenPhysical Examination in Respiratory SystemMarian0% (1)
- 8 - MRCP Part 1 - Recall May 2013Dokument28 Seiten8 - MRCP Part 1 - Recall May 2013Mohamed El-sayedNoch keine Bewertungen
- Thesis Topics in MicrobiologyDokument20 SeitenThesis Topics in MicrobiologyOlaoye50% (2)
- Gen. and Systemic Pathology Course Description & Lab. Manual Vol. 2 (AY 2021-2022) - Protected43Dokument245 SeitenGen. and Systemic Pathology Course Description & Lab. Manual Vol. 2 (AY 2021-2022) - Protected43Drashti kamodiaNoch keine Bewertungen
- Diseases - of - PleuraDokument110 SeitenDiseases - of - PleuraMohamed HefnyNoch keine Bewertungen
- Acute Bronchitis PDFDokument2 SeitenAcute Bronchitis PDFGenoMacaraanNoch keine Bewertungen
- Azithromycin Dosage Indications Adverse Effects NursingDokument1 SeiteAzithromycin Dosage Indications Adverse Effects NursingGrape JuiceNoch keine Bewertungen
- CV Ruby GuptaDokument4 SeitenCV Ruby GuptaAshish PatilNoch keine Bewertungen
- Nursing care plan SARSDokument5 SeitenNursing care plan SARSRhea Princess Tadeo88% (8)
- Bobcat Sambron Telehandler t40140 t40170 Spare Parts CatalogDokument22 SeitenBobcat Sambron Telehandler t40140 t40170 Spare Parts Catalogkathleenmullen211194fkn100% (37)
- Role of Procalcitonin in Diagnosis of Community Acquired Pneumonia in ChildrenDokument9 SeitenRole of Procalcitonin in Diagnosis of Community Acquired Pneumonia in ChildrenYasminNoch keine Bewertungen
- 1 Anatomi Dan Fisiologi Sistem RespirasiDokument9 Seiten1 Anatomi Dan Fisiologi Sistem RespirasiGhetsa ArNoch keine Bewertungen
- Respiratory Diseases in Children GuideDokument86 SeitenRespiratory Diseases in Children Guidemurugesh1969100% (1)
- Ursing Ervice: Cagayan Valley Medical CenterDokument13 SeitenUrsing Ervice: Cagayan Valley Medical CenterKirby C. CatulinNoch keine Bewertungen
- Mnemonics For Antibiotics-2Dokument10 SeitenMnemonics For Antibiotics-2totallyfakeusernameNoch keine Bewertungen
- Nurse Charting2Dokument7 SeitenNurse Charting2male nurseNoch keine Bewertungen
- Reviews: Population Genomics ofDokument16 SeitenReviews: Population Genomics ofRaul MolloNoch keine Bewertungen
- Streptococcus Pneumoniae S. PneumoniaeDokument18 SeitenStreptococcus Pneumoniae S. PneumoniaeadrianNoch keine Bewertungen
- Referat Batuk NurfitriDokument45 SeitenReferat Batuk NurfitribellabelbonNoch keine Bewertungen
- MRCP Revision NotesDokument14 SeitenMRCP Revision NotesSharanyMustafaNoch keine Bewertungen
- Pneumonii PedDokument19 SeitenPneumonii PedVeronica NefiruNoch keine Bewertungen
- Very Update Information About MedicineDokument13 SeitenVery Update Information About MedicinetriNoch keine Bewertungen
- Name - Perumal Sex: M - AgeDokument21 SeitenName - Perumal Sex: M - AgedrpravalkNoch keine Bewertungen
- Causes, Symptoms, and Treatment of PneumoniaDokument3 SeitenCauses, Symptoms, and Treatment of PneumoniaPedialy AvilesNoch keine Bewertungen
- Topnotch Microbiology Supertable by DR - Cocoy Calderon Jaffar Pineda Troy Soberano UPDATED NOVEMBER 2017Dokument16 SeitenTopnotch Microbiology Supertable by DR - Cocoy Calderon Jaffar Pineda Troy Soberano UPDATED NOVEMBER 2017Jaybee Sarmiento100% (1)