Das könnte Ihnen auch gefallen
- Presentation On Epistaxis in ChildrenDokument39 SeitenPresentation On Epistaxis in ChildrenAdditi SatyalNoch keine Bewertungen
- EPISTAXIS LectureDokument30 SeitenEPISTAXIS LectureDhienWhieNoch keine Bewertungen
- EpistaxisDokument33 SeitenEpistaxispaulyn ramosNoch keine Bewertungen
- Airway Obstruction Final2Dokument33 SeitenAirway Obstruction Final2Mahindra KumarNoch keine Bewertungen
- ENT Emergencies - DR Azwar Ridwan, SP - THT-KLDokument51 SeitenENT Emergencies - DR Azwar Ridwan, SP - THT-KLHayatul AkmaLiaNoch keine Bewertungen
- Ent Emergencies NKDokument39 SeitenEnt Emergencies NKGx NavinNoch keine Bewertungen
- Dr. Fifin Pradina Duhitatrissari SP - THT-KL FK Unisma/Rsi UnismaDokument49 SeitenDr. Fifin Pradina Duhitatrissari SP - THT-KL FK Unisma/Rsi Unisma216-104Yuda PerdanaNoch keine Bewertungen
- Ear InfectionDokument8 SeitenEar InfectionArt Christian Ramos100% (1)
- AtelektasisDokument15 SeitenAtelektasisMuhammad Ade RahmanNoch keine Bewertungen
- ScenarioDokument23 SeitenScenarioAakashNoch keine Bewertungen
- Stridor in Children: By: Maj Vishal Gaurav Moderator: DR A SethiDokument33 SeitenStridor in Children: By: Maj Vishal Gaurav Moderator: DR A SethiVishal GauravNoch keine Bewertungen
- Tracheostomy: Dr. Amar KumarDokument18 SeitenTracheostomy: Dr. Amar KumarSudhanshu ShekharNoch keine Bewertungen
- Antral WashDokument19 SeitenAntral WashRavi Bhushan SinghNoch keine Bewertungen
- Nasal Fractures: Trauma To NoseDokument38 SeitenNasal Fractures: Trauma To NoseSindhura ManjunathNoch keine Bewertungen
- Basic Sinus AnatomyDokument71 SeitenBasic Sinus AnatomyTalal AlanzyNoch keine Bewertungen
- Acute Otitis MediaDokument18 SeitenAcute Otitis MediaaliramzanNoch keine Bewertungen
- Lec.9 Sinonasal TumorsDokument25 SeitenLec.9 Sinonasal TumorsMariam QaisNoch keine Bewertungen
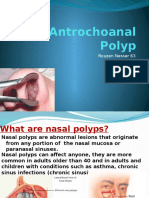
- Antrochoanal PolypDokument18 SeitenAntrochoanal PolypReem Eshra100% (1)
- ENT Emergency PresentationDokument135 SeitenENT Emergency PresentationshahiruddinNoch keine Bewertungen
- Anatomy and Physiology of The Conjunctiva: Presented by Arundhati Hatikakoty Bachelor of Optometry 3 Year Roll No-302Dokument43 SeitenAnatomy and Physiology of The Conjunctiva: Presented by Arundhati Hatikakoty Bachelor of Optometry 3 Year Roll No-302Vincentius Okta VidiandickaNoch keine Bewertungen
- TonsillectomyDokument4 SeitenTonsillectomyvalsamNoch keine Bewertungen
- Disorders of The Lacrimal Apparatus: Acute DacryocystitisDokument10 SeitenDisorders of The Lacrimal Apparatus: Acute DacryocystitisHariNoch keine Bewertungen
- ENT Examination of Nose.Dokument23 SeitenENT Examination of Nose.Kalyani TapreNoch keine Bewertungen
- Airway AdjunctsDokument17 SeitenAirway AdjunctsChannelGNoch keine Bewertungen
- Acute Laryngitis: Li SGD 21 LBM 5Dokument40 SeitenAcute Laryngitis: Li SGD 21 LBM 511juni09Noch keine Bewertungen
- Suctioning TracheaDokument24 SeitenSuctioning Trachealuis_chubee100% (1)
- ENT EmergencyDokument57 SeitenENT EmergencykylieverNoch keine Bewertungen
- Nasal Obstruction BookDokument7 SeitenNasal Obstruction BookChatradhar ChoudhuryNoch keine Bewertungen
- 20 - Common ENT Emergencies - FowlerDokument25 Seiten20 - Common ENT Emergencies - FowlerFrita Oktina WijayaNoch keine Bewertungen
- MnemonicsDokument11 SeitenMnemonicsanon-626602Noch keine Bewertungen
- Syncope: - Selvarathi KDokument27 SeitenSyncope: - Selvarathi KSelvarathi KandhaswamyNoch keine Bewertungen
- Tracheobronchial TreeDokument51 SeitenTracheobronchial TreeravishNoch keine Bewertungen
- DiphtheriaDokument22 SeitenDiphtheriaLovely Acabado TampocoNoch keine Bewertungen
- Seminar Asthma PDFDokument39 SeitenSeminar Asthma PDFAriff Mahdzub0% (1)
- Keratosis ObturansDokument12 SeitenKeratosis ObturansRahma LuthfaNoch keine Bewertungen
- Nasal TraumaDokument7 SeitenNasal TraumapoetwoNoch keine Bewertungen
- Acute Pyelonephritis Treatment & Management: Approach ConsiderationsDokument4 SeitenAcute Pyelonephritis Treatment & Management: Approach ConsiderationsPeter InocandoNoch keine Bewertungen
- Woman With PneumoniaDokument9 SeitenWoman With PneumoniaNohaira SADANGNoch keine Bewertungen
- Ear, Nose and Throat EmergenciesDokument3 SeitenEar, Nose and Throat Emergenciesfmta100% (1)
- External Ear Pathology - PresentationDokument25 SeitenExternal Ear Pathology - PresentationNipun MalhotraNoch keine Bewertungen
- External Ear DisordersDokument48 SeitenExternal Ear DisordershemaanandhyNoch keine Bewertungen
- TympanoplastyDokument4 SeitenTympanoplastyMelly Selvia ANoch keine Bewertungen
- Dr. Rosi - CPAPDokument65 SeitenDr. Rosi - CPAPtom24Noch keine Bewertungen
- ENT Teams A4 PDFDokument288 SeitenENT Teams A4 PDFEbrahim JuniorNoch keine Bewertungen
- IntubationDokument41 SeitenIntubationNice YouNoch keine Bewertungen
- Ent Emergencies Epistaxis (Nose Bleed)Dokument4 SeitenEnt Emergencies Epistaxis (Nose Bleed)Penny_Teoh_3451Noch keine Bewertungen
- Intro Head and NeckDokument74 SeitenIntro Head and NeckAuza Moses Ibrahim100% (2)
- ENT Quick ReviewDokument6 SeitenENT Quick ReviewWade100% (1)
- PARAQUAT POISIONING 3rd Block Imed COMPLIEDDokument15 SeitenPARAQUAT POISIONING 3rd Block Imed COMPLIEDMohil PratapNoch keine Bewertungen
- Cuerp Extra en Orl-Econa-Feb 2019Dokument10 SeitenCuerp Extra en Orl-Econa-Feb 2019surgeonyNoch keine Bewertungen
- Diagnosis & Treament: ShockDokument52 SeitenDiagnosis & Treament: ShockasepNoch keine Bewertungen
- Neurological Assessment PDFDokument52 SeitenNeurological Assessment PDFJosephine George JojoNoch keine Bewertungen
- Ent Ospe Badhahin v1 7 PDFDokument26 SeitenEnt Ospe Badhahin v1 7 PDFWasi OsmanNoch keine Bewertungen
- Csom (TT)Dokument24 SeitenCsom (TT)SamirNoch keine Bewertungen
- Le Fort II Fracture (Pyramidal Fracture)Dokument116 SeitenLe Fort II Fracture (Pyramidal Fracture)Zain A. ShimariNoch keine Bewertungen
- Csom 090615124432 Phpapp01Dokument36 SeitenCsom 090615124432 Phpapp01Ibrahim QuadriNoch keine Bewertungen
- Perichondritis PinnaDokument2 SeitenPerichondritis PinnaAnish RajNoch keine Bewertungen
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- Assaignment Title: Causes, Work Up & Management of Epistaxis Discipline: MBBSDokument11 SeitenAssaignment Title: Causes, Work Up & Management of Epistaxis Discipline: MBBSJahanzaib SaeedNoch keine Bewertungen
- Diabetes and Its Permanent Cure With Homeopathic Medicines - DRDokument28 SeitenDiabetes and Its Permanent Cure With Homeopathic Medicines - DRkrishna kumar67% (3)
- Respiratory Therapist Licensure Examination Passer"s ListDokument7 SeitenRespiratory Therapist Licensure Examination Passer"s ListzoomscannerNoch keine Bewertungen
- Hypothesis ProblemsDokument7 SeitenHypothesis Problemsrj0% (1)
- Children's Depression Inventory CDI™Dokument2 SeitenChildren's Depression Inventory CDI™ManickaSaravanan27% (11)
- Insulin IndexDokument13 SeitenInsulin IndexbookbookpdfNoch keine Bewertungen
- Eyelid Surgery Los AngelesDokument2 SeitenEyelid Surgery Los AngelesVeronica HinmanNoch keine Bewertungen
- Diagnosis and Treatment of Root PerforationsDokument13 SeitenDiagnosis and Treatment of Root PerforationsNico LucaciNoch keine Bewertungen
- Anaesthesia TMJ Pain Orthognathic Pathology ReconstructionDokument220 SeitenAnaesthesia TMJ Pain Orthognathic Pathology ReconstructionMohammed Qasim Al-Watary67% (3)
- National Antibiotic Guideline 2014 Full Versionjun2015 - 1 PDFDokument247 SeitenNational Antibiotic Guideline 2014 Full Versionjun2015 - 1 PDFfghjNoch keine Bewertungen
- Clean EatingDokument92 SeitenClean EatingLia Vágvölgyi100% (1)
- Smoking Updated PDFDokument5 SeitenSmoking Updated PDFJoshua BoncodinNoch keine Bewertungen
- A Comparative Clinical Study To Evaluate The Efficacy of Koshataki Ksharasutra in The Management of Bhagandara With Special Reference To Fistula in AnoDokument7 SeitenA Comparative Clinical Study To Evaluate The Efficacy of Koshataki Ksharasutra in The Management of Bhagandara With Special Reference To Fistula in AnoEditor IJTSRDNoch keine Bewertungen
- Macedo 2019Dokument6 SeitenMacedo 2019cpfisioNoch keine Bewertungen
- Material Safety Data Sheet: 1 IdentificationDokument6 SeitenMaterial Safety Data Sheet: 1 IdentificationGio Ibarra MolinaNoch keine Bewertungen
- HYDRALAZINE HYDROCHLORIDE - (Apresoline)Dokument1 SeiteHYDRALAZINE HYDROCHLORIDE - (Apresoline)wen_pilNoch keine Bewertungen
- NCP PainDokument4 SeitenNCP PainFlauros Ryu JabienNoch keine Bewertungen
- Montano NCP TbiDokument6 SeitenMontano NCP TbiKarl Angelo MontanoNoch keine Bewertungen
- WarfarinDokument10 SeitenWarfarinMar Ordanza100% (1)
- Konker AbstractDokument39 SeitenKonker AbstractWigunaNoch keine Bewertungen
- The Science of Addiction (Drugs and The Brain)Dokument84 SeitenThe Science of Addiction (Drugs and The Brain)cacker4140100% (1)
- Removable AppliancesDokument32 SeitenRemovable AppliancesmegamarwaNoch keine Bewertungen
- Understanding HypokalemiaDokument4 SeitenUnderstanding HypokalemiaAudrey Leonar100% (1)
- Acute Circulatory FailureDokument21 SeitenAcute Circulatory FailureachyutsharmaNoch keine Bewertungen
- Antibiotics Guide 2013Dokument30 SeitenAntibiotics Guide 2013Stefani NoviliaNoch keine Bewertungen
- PsychoanalysisDokument5 SeitenPsychoanalysisapi-249311611Noch keine Bewertungen
- Catheter Related Bloodstream Infection (CRBSI)Dokument36 SeitenCatheter Related Bloodstream Infection (CRBSI)aringkinkingNoch keine Bewertungen
- Electric Field Distribution in Biological Tissues For Various Electrode Configurations - A FEMLAB StudyDokument5 SeitenElectric Field Distribution in Biological Tissues For Various Electrode Configurations - A FEMLAB StudyxlippyfingersNoch keine Bewertungen
- Cruze: 2014 Silverado Is Here!Dokument24 SeitenCruze: 2014 Silverado Is Here!Sherman Publications, Inc.100% (1)
- Dex in USGDokument8 SeitenDex in USGvaishaliNoch keine Bewertungen
- Perioperative Nursing 50 ItemsDokument4 SeitenPerioperative Nursing 50 Itemssan maeNoch keine Bewertungen