Das könnte Ihnen auch gefallen
- Hypersensitivities Dermatitis Atopic PDFDokument70 SeitenHypersensitivities Dermatitis Atopic PDFSarahUtamiSr.Noch keine Bewertungen
- Myocarditis Due To Systemic Lupus Erythematosus Associated With Cardiogenic ShockDokument3 SeitenMyocarditis Due To Systemic Lupus Erythematosus Associated With Cardiogenic ShockAkbar IskandarNoch keine Bewertungen
- Cardiogenic Shock PediatricDokument9 SeitenCardiogenic Shock PediatricAkbar IskandarNoch keine Bewertungen
- Laporan Sesak Kelompok A6Dokument66 SeitenLaporan Sesak Kelompok A6Akbar IskandarNoch keine Bewertungen
- LAporan Kasus Sesak Kelompok A2Dokument57 SeitenLAporan Kasus Sesak Kelompok A2Akbar IskandarNoch keine Bewertungen
- AustralianTriageScales Guidelines PDFDokument10 SeitenAustralianTriageScales Guidelines PDFMaryantiNoch keine Bewertungen
- B3Dokument45 SeitenB3Akbar IskandarNoch keine Bewertungen
- Laporan Sesak Kelompok A7Dokument47 SeitenLaporan Sesak Kelompok A7Akbar IskandarNoch keine Bewertungen
- Laporan Sesak Kelompok B2Dokument27 SeitenLaporan Sesak Kelompok B2Akbar IskandarNoch keine Bewertungen
- Laporan Sesak Kelompok A7Dokument50 SeitenLaporan Sesak Kelompok A7Akbar IskandarNoch keine Bewertungen
- Sistem Respirasi Sesak Napas: Problem Based LearningDokument61 SeitenSistem Respirasi Sesak Napas: Problem Based LearningAkbar IskandarNoch keine Bewertungen
- Laporan Sesak Kelompok A5Dokument42 SeitenLaporan Sesak Kelompok A5Akbar IskandarNoch keine Bewertungen
- CHF Nyha IV Ec CHDDokument34 SeitenCHF Nyha IV Ec CHDAkbar IskandarNoch keine Bewertungen
- CHF Ec CadDokument17 SeitenCHF Ec CadAkbar IskandarNoch keine Bewertungen
- Laporan Sesak Kelompok A1Dokument42 SeitenLaporan Sesak Kelompok A1Akbar IskandarNoch keine Bewertungen
- Congestive Heart Failure Et Causa Mitral InsuficiencyDokument43 SeitenCongestive Heart Failure Et Causa Mitral InsuficiencyAkbar IskandarNoch keine Bewertungen
- Supraventricular Tachycardia PresentationDokument31 SeitenSupraventricular Tachycardia PresentationAkbar IskandarNoch keine Bewertungen
- CHF NYHA III-IV Ec MSDokument28 SeitenCHF NYHA III-IV Ec MSAkbar IskandarNoch keine Bewertungen
- CHF NYHA IV ec. MS ec. RHDDokument37 SeitenCHF NYHA IV ec. MS ec. RHDAkbar IskandarNoch keine Bewertungen
- CHF NYHA IV Ec CADDokument38 SeitenCHF NYHA IV Ec CADAkbar IskandarNoch keine Bewertungen
- CHF NYHA IV Ec Mitral RegugitationDokument38 SeitenCHF NYHA IV Ec Mitral RegugitationAkbar IskandarNoch keine Bewertungen
- CHF NYHA III-IV Ec. CADDokument25 SeitenCHF NYHA III-IV Ec. CADAkbar IskandarNoch keine Bewertungen
- CHF NYHA IV Ec Mitral StenosisDokument31 SeitenCHF NYHA IV Ec Mitral StenosisAkbar Iskandar100% (1)
- Complete Heart Block-Chf Nyha III Ec Aortic StenosisDokument34 SeitenComplete Heart Block-Chf Nyha III Ec Aortic StenosisAkbar IskandarNoch keine Bewertungen
- CHF Nyha IV Ec Severe MRDokument42 SeitenCHF Nyha IV Ec Severe MRAkbar IskandarNoch keine Bewertungen
- Atrial Septal Defect (ASD)Dokument22 SeitenAtrial Septal Defect (ASD)Akbar Iskandar100% (1)
- CHF NYHA IV Ec Susp. MSDokument30 SeitenCHF NYHA IV Ec Susp. MSAkbar IskandarNoch keine Bewertungen
- CHF E.C. ASD (Irma)Dokument37 SeitenCHF E.C. ASD (Irma)Akbar IskandarNoch keine Bewertungen
- Anterior Wall Myocardial IschemiaDokument32 SeitenAnterior Wall Myocardial IschemiaAkbar IskandarNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Cme Bronchial AsthmaDokument28 SeitenCme Bronchial AsthmaameerabestNoch keine Bewertungen
- Cesar - Evaluation - ImciDokument3 SeitenCesar - Evaluation - ImcikdfhjfhfNoch keine Bewertungen
- Asthma PamphletDokument2 SeitenAsthma Pamphletjeng214Noch keine Bewertungen
- Provide chest physiotherapy to mobilize secretions and improve lung expansion and ventilationDokument19 SeitenProvide chest physiotherapy to mobilize secretions and improve lung expansion and ventilationMonica BorjaNoch keine Bewertungen
- NCLEX RN Practice Questions 17Dokument6 SeitenNCLEX RN Practice Questions 17RI NANoch keine Bewertungen
- First Aid Kit HomeoDokument12 SeitenFirst Aid Kit HomeoBelegan CrengutaNoch keine Bewertungen
- Item Prek OotDokument9 SeitenItem Prek OotAmaliya 23Noch keine Bewertungen
- Pulmonary and Critical Care MnemonicsDokument10 SeitenPulmonary and Critical Care MnemonicsnmahpbooksNoch keine Bewertungen
- Tuberculinum HerscuDokument42 SeitenTuberculinum Herscupanniyin selvanNoch keine Bewertungen
- TUBERCULOSISDokument9 SeitenTUBERCULOSISRahma WatiNoch keine Bewertungen
- Rumentalia Sulistini Aguscik Maria Ulfa, Politeknik Kesehatan Kemmenkes Palembang, Sumatera Selatan, IndonesiaDokument7 SeitenRumentalia Sulistini Aguscik Maria Ulfa, Politeknik Kesehatan Kemmenkes Palembang, Sumatera Selatan, IndonesiaCristina HeatubunNoch keine Bewertungen
- OtcDokument9 SeitenOtcChrissie100% (1)
- TM 4750-15-1 - ADokument112 SeitenTM 4750-15-1 - ABrian Molsbee100% (1)
- Care Plan FaringitisDokument63 SeitenCare Plan FaringitisEnerolisa ParedesNoch keine Bewertungen
- NCP (Ineffective Airway Clearance, URTI)Dokument6 SeitenNCP (Ineffective Airway Clearance, URTI)Jenny AjocNoch keine Bewertungen
- Labeling OTC Human Drug Products Small Entity Compliance GuideDokument24 SeitenLabeling OTC Human Drug Products Small Entity Compliance GuideMohammed Shamiul ShahidNoch keine Bewertungen
- Pharmacology 9Dokument51 SeitenPharmacology 9anjie kamidNoch keine Bewertungen
- NCLEX Questions PulmDokument27 SeitenNCLEX Questions PulmAnthony Hawley100% (2)
- Zang-Fu Syndrome Differentiation - UERMDokument113 SeitenZang-Fu Syndrome Differentiation - UERMNathaniel P. Peralta0% (1)
- CopdDokument89 SeitenCopdVijayalaxmi KathareNoch keine Bewertungen
- Cough PathophysiolgyDokument5 SeitenCough PathophysiolgyAudini BerbasariNoch keine Bewertungen
- Home Remedies For PneumoniaDokument15 SeitenHome Remedies For PneumoniaAljunBaetiongDiazNoch keine Bewertungen
- The Six Pernicious InfluencesDokument2 SeitenThe Six Pernicious InfluencesredleberaNoch keine Bewertungen
- Methods of ResearchDokument35 SeitenMethods of ResearchGerik JavonilloNoch keine Bewertungen
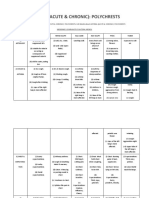
- Asthma (Acute & Chronic) : PolychrestsDokument14 SeitenAsthma (Acute & Chronic) : Polychrestss.s.r.k.m. guptaNoch keine Bewertungen
- Diseases and Their RemediesDokument191 SeitenDiseases and Their Remediesnymufti97% (31)
- Waking Up Gasping For Air Anxiety, Falling Asleep, Acid RefluxDokument1 SeiteWaking Up Gasping For Air Anxiety, Falling Asleep, Acid RefluxAstra CardinalNoch keine Bewertungen
- Chinese Herbal Formulas: A Clinical Handbook: 2nd EditionDokument17 SeitenChinese Herbal Formulas: A Clinical Handbook: 2nd EditionJustina Le Coq0% (1)
- CA RationaleDokument39 SeitenCA RationaleSeirah Distor MartinezNoch keine Bewertungen
- Pathophysiology of AsthmaDokument71 SeitenPathophysiology of AsthmaChin ChanNoch keine Bewertungen