Das könnte Ihnen auch gefallen
- LEC1 - Definition & Scope of Hematology To Red Blood Cell StudiesDokument11 SeitenLEC1 - Definition & Scope of Hematology To Red Blood Cell StudiessuperbbloomNoch keine Bewertungen
- Circulatory SystemDokument74 SeitenCirculatory SystemMICHAEL AFIADENYONoch keine Bewertungen
- BloodDokument56 SeitenBloodGail Justine Chongco GonzalesNoch keine Bewertungen
- Week 14 - Blood and Hematopoeitic SystemDokument47 SeitenWeek 14 - Blood and Hematopoeitic SystemGeevee Naganag VentulaNoch keine Bewertungen
- University of Guyana Health Sciences FacultyDokument44 SeitenUniversity of Guyana Health Sciences FacultySatrohan SurjnarineNoch keine Bewertungen
- PSG 712 Blood-1Dokument54 SeitenPSG 712 Blood-1preciousNoch keine Bewertungen
- Cardiovascular System: BloodDokument5 SeitenCardiovascular System: BloodKoh Yen SinNoch keine Bewertungen
- Blood Summary NotesDokument4 SeitenBlood Summary NotesLaura FernandezNoch keine Bewertungen
- Power Point Presentation Blood Cells: Name: Reg - No: ClassDokument20 SeitenPower Point Presentation Blood Cells: Name: Reg - No: ClassAnonymous L96u5itNoch keine Bewertungen
- Heamatology Chapter 1Dokument38 SeitenHeamatology Chapter 1Taima'a AlamaratNoch keine Bewertungen
- DarahDokument48 SeitenDarahTya DwiNoch keine Bewertungen
- CVS BloodDokument39 SeitenCVS BloodMohan GuptaNoch keine Bewertungen
- Chapter 4 Blood Coagulation and Coagulation Disorders _32f6d4d0c67589df3863ad91f445f357Dokument27 SeitenChapter 4 Blood Coagulation and Coagulation Disorders _32f6d4d0c67589df3863ad91f445f357daisysintszwaiNoch keine Bewertungen
- Biology 12 - Chapter 11 - Blood - Chapter Notes: Here Is A Micrographs Showing Formed Elements in Human BloodDokument7 SeitenBiology 12 - Chapter 11 - Blood - Chapter Notes: Here Is A Micrographs Showing Formed Elements in Human BloodChan KarlokNoch keine Bewertungen
- Blood: Group 1Dokument25 SeitenBlood: Group 1Arian May MarcosNoch keine Bewertungen
- Darah: Dr. Yetty Machrina Bagian Fisiologi FK UsuDokument44 SeitenDarah: Dr. Yetty Machrina Bagian Fisiologi FK UsuMyst AngelNoch keine Bewertungen
- Blood Components and FunctionsDokument10 SeitenBlood Components and FunctionsShiela Mae SagayoNoch keine Bewertungen
- The Cardiovascular SystemDokument79 SeitenThe Cardiovascular Systemhed-ikaquinoNoch keine Bewertungen
- Chapter 19 - BloodDokument5 SeitenChapter 19 - Bloodtomorrow.today.yesterday .yesterdayNoch keine Bewertungen
- Hematology Notes LectureDokument7 SeitenHematology Notes LectureMiles Angel LacayNoch keine Bewertungen
- Hematologic DisordersDokument30 SeitenHematologic DisordersUday Kumar100% (1)
- 1-Blood Composition and FunctionDokument43 Seiten1-Blood Composition and FunctionKaleem Mohammad100% (2)
- Blood: - The Only Fluid Tissue in The Human Body - Classified As A Connective TissueDokument39 SeitenBlood: - The Only Fluid Tissue in The Human Body - Classified As A Connective TissueJorNoch keine Bewertungen
- Histology of Blood CellsDokument80 SeitenHistology of Blood CellsKamal AhmedNoch keine Bewertungen
- Chapter 17 Anatomy and Physiology NotesDokument10 SeitenChapter 17 Anatomy and Physiology NotesZachary WatsonNoch keine Bewertungen
- Circulatory System and Parts 1Dokument38 SeitenCirculatory System and Parts 1Atasha Ivory RagragioNoch keine Bewertungen
- BLOODDokument12 SeitenBLOOD- HY0ENGJUNNoch keine Bewertungen
- Chapter 30 Nursing Assessment Hematologic SystemDokument14 SeitenChapter 30 Nursing Assessment Hematologic Systemmedic-24100% (1)
- Components of Blood - Red Blood Cells, White Blood Cells, and PlateletsDokument20 SeitenComponents of Blood - Red Blood Cells, White Blood Cells, and PlateletsVishal SharmaNoch keine Bewertungen
- Blood and Its Components-NotesDokument10 SeitenBlood and Its Components-NotesKelvin RequenaNoch keine Bewertungen
- The Circulatory System 2. 1 Composition and Function of BloodDokument29 SeitenThe Circulatory System 2. 1 Composition and Function of BlooddevNoch keine Bewertungen
- Blood Physical PropertiesDokument38 SeitenBlood Physical PropertiesYvonne Kath SmitchNoch keine Bewertungen
- Unit 2-Blood Guided NotesDokument5 SeitenUnit 2-Blood Guided NotesJeanette IrambonaNoch keine Bewertungen
- Darah: Dr. Yetty Machrina Bagian Fisiologi FK UsuDokument44 SeitenDarah: Dr. Yetty Machrina Bagian Fisiologi FK Usukiki rawitriNoch keine Bewertungen
- Blood Composition and FormationDokument27 SeitenBlood Composition and Formationchandu ranaNoch keine Bewertungen
- Chapter 10 Blood AnatomyDokument5 SeitenChapter 10 Blood AnatomyChiara Mae NiñalNoch keine Bewertungen
- Human Anatomy & Physiology: Blood & HematologyDokument13 SeitenHuman Anatomy & Physiology: Blood & HematologyAymen OmerNoch keine Bewertungen
- Blood PDFDokument55 SeitenBlood PDFlorrainebarandonNoch keine Bewertungen
- Chap1 Transportform5 120218082802 Phpapp01Dokument107 SeitenChap1 Transportform5 120218082802 Phpapp01Santhiya MadhavanNoch keine Bewertungen
- Fisiologi Cairan Tubuh & Darah: Dr. Nindya Aryanty, M.Med - EdDokument43 SeitenFisiologi Cairan Tubuh & Darah: Dr. Nindya Aryanty, M.Med - EdIman TaufiqNoch keine Bewertungen
- Blood and Its ComponentsDokument22 SeitenBlood and Its ComponentsSudhir Singh100% (1)
- CH 15 BloodDokument6 SeitenCH 15 Bloodsann1992Noch keine Bewertungen
- Blood and Its FunctionsDokument47 SeitenBlood and Its FunctionsMatende husseinNoch keine Bewertungen
- Biology ReviewerDokument5 SeitenBiology Reviewer13l4nk17Noch keine Bewertungen
- Darah Dan LimfatikDokument55 SeitenDarah Dan Limfatikadisty sncNoch keine Bewertungen
- The Circulatory System - 4th FormDokument25 SeitenThe Circulatory System - 4th FormKristal CampbellNoch keine Bewertungen
- Lecture 9 CVSDokument118 SeitenLecture 9 CVSMuhammad Abbas WaliNoch keine Bewertungen
- Blood: - Enzymes, E.G. Certain Clotting FactorsDokument14 SeitenBlood: - Enzymes, E.G. Certain Clotting FactorsDerrick kinyaNoch keine Bewertungen
- Fisiologi DARAHDokument31 SeitenFisiologi DARAHTririn RinantiNoch keine Bewertungen
- Body FluidsDokument14 SeitenBody FluidsathuNoch keine Bewertungen
- Introduction to Blood Composition and HaemopoiesisDokument119 SeitenIntroduction to Blood Composition and HaemopoiesisShamsuddeen UsmanNoch keine Bewertungen
- Blood ReviewDokument13 SeitenBlood ReviewDeleted AccountNoch keine Bewertungen
- Ematology: MLT Department 2 - Stage Theoretical Part/ Lecture No. 1 by Dilgeer Ahmed KalariDokument24 SeitenEmatology: MLT Department 2 - Stage Theoretical Part/ Lecture No. 1 by Dilgeer Ahmed Kalariphotocopy beshaNoch keine Bewertungen
- Blood HBDokument31 SeitenBlood HBBHUWAN BASKOTANoch keine Bewertungen
- Characteristics and Functions of Blood ComponentsDokument51 SeitenCharacteristics and Functions of Blood ComponentssamayaNoch keine Bewertungen
- 1 BloodDokument31 Seiten1 BloodSuchana AcNoch keine Bewertungen
- ANAT - Unit 3 - Blood Composition NotesDokument28 SeitenANAT - Unit 3 - Blood Composition NotesJaren Balbal0% (1)
- The Essence of Life: A Concise Overview of Blood Composition and FunctionsDokument46 SeitenThe Essence of Life: A Concise Overview of Blood Composition and FunctionsGrape JuiceNoch keine Bewertungen
- Blood PropertiesDokument38 SeitenBlood PropertiesShubham BhandareNoch keine Bewertungen
- Digestive System: Stomach and Small Intestine FunctionsDokument56 SeitenDigestive System: Stomach and Small Intestine FunctionsJerilee SoCute WattsNoch keine Bewertungen
- SkinDokument43 SeitenSkinFhen Farrel100% (1)
- Skin Diseases Disorders ConditionsDokument104 SeitenSkin Diseases Disorders ConditionsJerilee SoCute WattsNoch keine Bewertungen
- PDFDokument64 SeitenPDFJerilee SoCute WattsNoch keine Bewertungen
- Digestive SystemDokument48 SeitenDigestive SystemJerilee SoCute WattsNoch keine Bewertungen
- The Digestive System Part 1Dokument28 SeitenThe Digestive System Part 1Jerilee SoCute WattsNoch keine Bewertungen
- Urinary SystemDokument105 SeitenUrinary SystemJerilee SoCute WattsNoch keine Bewertungen
- The Circulatory System-: TransportDokument13 SeitenThe Circulatory System-: TransportJerilee SoCute WattsNoch keine Bewertungen
- CV SYSTEM ANATOMYDokument42 SeitenCV SYSTEM ANATOMYJerilee SoCute WattsNoch keine Bewertungen
- Lecture 21 - Respiratory SystemDokument59 SeitenLecture 21 - Respiratory SystemSkyBirdNoch keine Bewertungen
- The Lymphatic SystemDokument50 SeitenThe Lymphatic SystemJerilee SoCute Watts100% (1)
- Reproductive SystemDokument80 SeitenReproductive SystemJerilee SoCute WattsNoch keine Bewertungen
- The Conducting System of The HeartDokument37 SeitenThe Conducting System of The HeartJerilee SoCute WattsNoch keine Bewertungen
- Respiratory System Anatomy and Functions EX36Dokument57 SeitenRespiratory System Anatomy and Functions EX36royanirudh99Noch keine Bewertungen
- Reproduction and DevelopmentDokument53 SeitenReproduction and DevelopmentJerilee SoCute WattsNoch keine Bewertungen
- The Digestive System EssayDokument3 SeitenThe Digestive System EssayJerilee SoCute Watts0% (1)
- Respiratory System 2Dokument39 SeitenRespiratory System 2Jerilee SoCute WattsNoch keine Bewertungen
- Reproduction NotesDokument20 SeitenReproduction NotesMario BaemamentengNoch keine Bewertungen
- Review Questions - Heart Anatomy & PhysiologyDokument1 SeiteReview Questions - Heart Anatomy & PhysiologyJerilee SoCute WattsNoch keine Bewertungen
- Pulmonary and Systemic CircuitsDokument38 SeitenPulmonary and Systemic CircuitsJerilee SoCute WattsNoch keine Bewertungen
- Reproductive System DisordersDokument62 SeitenReproductive System DisordersJerilee SoCute Watts100% (2)
- Respiratory System 1Dokument29 SeitenRespiratory System 1Jerilee SoCute WattsNoch keine Bewertungen
- Human ReproductionDokument42 SeitenHuman ReproductionAliDarimiKRNoch keine Bewertungen
- Brain Respiratory Centers & Control MechanismsDokument36 SeitenBrain Respiratory Centers & Control MechanismsJerilee SoCute WattsNoch keine Bewertungen
- Reproduction Summary NotesDokument16 SeitenReproduction Summary NotesJerilee SoCute WattsNoch keine Bewertungen
- Lecture 1 Cardiovascular SystemDokument70 SeitenLecture 1 Cardiovascular SystemJerilee SoCute WattsNoch keine Bewertungen
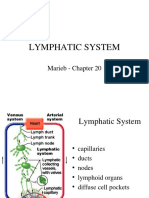
- Lymphatic System: Marieb Chapter 20Dokument22 SeitenLymphatic System: Marieb Chapter 20Jerilee SoCute WattsNoch keine Bewertungen
- Unit 6 OsmolarityDokument59 SeitenUnit 6 Osmolaritykrystal1994Noch keine Bewertungen
- Lecture 2 Cardiovascular SystemDokument70 SeitenLecture 2 Cardiovascular SystemJerilee SoCute WattsNoch keine Bewertungen
- Platelets and HemostasisDokument19 SeitenPlatelets and HemostasisJerilee SoCute WattsNoch keine Bewertungen
- A Princess of Mars Part 3Dokument4 SeitenA Princess of Mars Part 3Sheila Inca100% (1)
- Gabinete STS Activity1Dokument2 SeitenGabinete STS Activity1Anthony GabineteNoch keine Bewertungen
- Methods to estimate stakeholder views of sustainabilityDokument7 SeitenMethods to estimate stakeholder views of sustainabilityAlireza FatemiNoch keine Bewertungen
- Crystallizers: Chapter 16 Cost Accounting and Capital Cost EstimationDokument1 SeiteCrystallizers: Chapter 16 Cost Accounting and Capital Cost EstimationDeiver Enrique SampayoNoch keine Bewertungen
- Duca Industries March 2023 pay slip for Dipankar MondalDokument1 SeiteDuca Industries March 2023 pay slip for Dipankar MondalPritam GoswamiNoch keine Bewertungen
- Employee Confidentiality and Non-Disclosure AgreementDokument5 SeitenEmployee Confidentiality and Non-Disclosure AgreementshamoojeeNoch keine Bewertungen
- Job Order Costing: Patrick Louie E. Reyes, CTT, Micb, Rca, CpaDokument45 SeitenJob Order Costing: Patrick Louie E. Reyes, CTT, Micb, Rca, CpaClaudette Clemente100% (1)
- IQ CommandDokument6 SeitenIQ CommandkuoliusNoch keine Bewertungen
- Prlude No BWV in C MinorDokument3 SeitenPrlude No BWV in C MinorFrédéric LemaireNoch keine Bewertungen
- Get Oracle Order DetailsDokument4 SeitenGet Oracle Order Detailssiva_lordNoch keine Bewertungen
- Hydraulics Engineering Course OverviewDokument35 SeitenHydraulics Engineering Course Overviewahmad akramNoch keine Bewertungen
- Uniform-Section Disk Spring AnalysisDokument10 SeitenUniform-Section Disk Spring Analysischristos032Noch keine Bewertungen
- Chromate Free CoatingsDokument16 SeitenChromate Free CoatingsbaanaadiNoch keine Bewertungen
- Corporate Governance, Corporate Profitability Toward Corporate Social Responsibility Disclosure and Corporate Value (Comparative Study in Indonesia, China and India Stock Exchange in 2013-2016) .Dokument18 SeitenCorporate Governance, Corporate Profitability Toward Corporate Social Responsibility Disclosure and Corporate Value (Comparative Study in Indonesia, China and India Stock Exchange in 2013-2016) .Lia asnamNoch keine Bewertungen
- Pfr140 User ManualDokument4 SeitenPfr140 User ManualOanh NguyenNoch keine Bewertungen
- Mounting InstructionDokument1 SeiteMounting InstructionAkshay GargNoch keine Bewertungen
- Todo Matic PDFDokument12 SeitenTodo Matic PDFSharrife JNoch keine Bewertungen
- PNBONE_mPassbook_134611_6-4-2024_13-4-2024_0053XXXXXXXX00 (1) (1)Dokument3 SeitenPNBONE_mPassbook_134611_6-4-2024_13-4-2024_0053XXXXXXXX00 (1) (1)imtiyaz726492Noch keine Bewertungen
- Annual Plan 1st GradeDokument3 SeitenAnnual Plan 1st GradeNataliaMarinucciNoch keine Bewertungen
- AD Chemicals - Freeze-Flash PointDokument4 SeitenAD Chemicals - Freeze-Flash Pointyb3yonnayNoch keine Bewertungen
- CENG 5503 Intro to Steel & Timber StructuresDokument37 SeitenCENG 5503 Intro to Steel & Timber StructuresBern Moses DuachNoch keine Bewertungen
- Statistical Quality Control, 7th Edition by Douglas C. Montgomery. 1Dokument76 SeitenStatistical Quality Control, 7th Edition by Douglas C. Montgomery. 1omerfaruk200141Noch keine Bewertungen
- Service Manual: Precision SeriesDokument32 SeitenService Manual: Precision SeriesMoises ShenteNoch keine Bewertungen
- Tutorial 1 Discussion Document - Batch 03Dokument4 SeitenTutorial 1 Discussion Document - Batch 03Anindya CostaNoch keine Bewertungen
- Special Power of Attorney: Benedict Joseph M. CruzDokument1 SeiteSpecial Power of Attorney: Benedict Joseph M. CruzJson GalvezNoch keine Bewertungen
- Dermatology Study Guide 2023-IvDokument7 SeitenDermatology Study Guide 2023-IvUnknown ManNoch keine Bewertungen
- NLP Business Practitioner Certification Course OutlineDokument11 SeitenNLP Business Practitioner Certification Course OutlineabobeedoNoch keine Bewertungen
- Nagina Cotton Mills Annual Report 2007Dokument44 SeitenNagina Cotton Mills Annual Report 2007Sonia MukhtarNoch keine Bewertungen
- Mil STD 2154Dokument44 SeitenMil STD 2154Muh SubhanNoch keine Bewertungen
- Final Year Project (Product Recommendation)Dokument33 SeitenFinal Year Project (Product Recommendation)Anurag ChakrabortyNoch keine Bewertungen