Das könnte Ihnen auch gefallen
- Boiler Explosion Case Study2Dokument2 SeitenBoiler Explosion Case Study2Hoang ThangNoch keine Bewertungen
- Confined Vapor and Gas Fatalities in Upstream OperationsDokument16 SeitenConfined Vapor and Gas Fatalities in Upstream Operationssmithyry2014Noch keine Bewertungen
- Hse MS SlidesDokument32 SeitenHse MS SlidesEneyo Victor100% (1)
- Nebosh PSM BrochureDokument1 SeiteNebosh PSM BrochureKannan JaganNoch keine Bewertungen
- PSM ComplianceDokument35 SeitenPSM CompliancejishnusajiNoch keine Bewertungen
- 51 Confined SpaceDokument1 Seite51 Confined SpaceAnonymous ANmMebffKRNoch keine Bewertungen
- h2s Instructor 1Dokument96 Seitenh2s Instructor 1SafetymanmarkNoch keine Bewertungen
- 1 - ERP - CrisisDokument124 Seiten1 - ERP - Crisisamira_zainal92Noch keine Bewertungen
- Whip ChecksDokument2 SeitenWhip ChecksSusin Lim100% (1)
- 10 Industrial Accidents Where Poor Shift Handover Was A Contributory FactorDokument2 Seiten10 Industrial Accidents Where Poor Shift Handover Was A Contributory FactorsgraureNoch keine Bewertungen
- User-Manual-25262Compressed Gas Cylinders PowerPointDokument20 SeitenUser-Manual-25262Compressed Gas Cylinders PowerPointMohammed NaseeruddinNoch keine Bewertungen
- NEBOSH HSE Certificate in Process Safety Management: Course BenefitsDokument1 SeiteNEBOSH HSE Certificate in Process Safety Management: Course BenefitsNational Institute of Safety EngineersNoch keine Bewertungen
- CONTROL SHEETS & FORMS permit guideDokument3 SeitenCONTROL SHEETS & FORMS permit guideHenry WoartNoch keine Bewertungen
- Hazard of Sulfuric AcidDokument3 SeitenHazard of Sulfuric AcidAlisameimeiNoch keine Bewertungen
- Ract No. (If Applicable) :si Gnature: DateDokument8 SeitenRact No. (If Applicable) :si Gnature: DatetaldienahmadNoch keine Bewertungen
- TBT Press - Test.Dokument2 SeitenTBT Press - Test.John Vem BansagNoch keine Bewertungen
- Nitrogen Info Pack 2011Dokument18 SeitenNitrogen Info Pack 2011Nizami ShirinovNoch keine Bewertungen
- Employers LiabilityDokument43 SeitenEmployers LiabilitysaifulmuslimzNoch keine Bewertungen
- Confined Space - Introduction: Canadian Government Departments Responsible For OH&S Confined Space - ProgramDokument7 SeitenConfined Space - Introduction: Canadian Government Departments Responsible For OH&S Confined Space - ProgramAnge JuanNoch keine Bewertungen
- Breathe Right!Dokument44 SeitenBreathe Right!Safety and Health magazineNoch keine Bewertungen
- 059 Vacuum Truck SafetyDokument6 Seiten059 Vacuum Truck Safetyichal_zaidanNoch keine Bewertungen
- HYDROBLASTER SAFETYDokument2 SeitenHYDROBLASTER SAFETYHamza Nouman100% (2)
- Nitrogen DangerDokument27 SeitenNitrogen DangerMạnh Bùi100% (1)
- Stress at Workplace Group 10Dokument52 SeitenStress at Workplace Group 10Liew Sam TatNoch keine Bewertungen
- Flixborough (UK) 197402 0Dokument13 SeitenFlixborough (UK) 197402 0Emma Slater100% (1)
- Emirates ERM Abu Dhabi Process Safety Management Training MethodologyDokument5 SeitenEmirates ERM Abu Dhabi Process Safety Management Training MethodologyShailendraNoch keine Bewertungen
- Hot Work Permit ProceduresDokument9 SeitenHot Work Permit ProceduresFerdinand M. TurbanosNoch keine Bewertungen
- HSSE Training Manual Chapter SummariesDokument47 SeitenHSSE Training Manual Chapter SummariesEneyo VictorNoch keine Bewertungen
- Life Saving Rules Speaker Support Pack Jan 2012Dokument33 SeitenLife Saving Rules Speaker Support Pack Jan 2012Muhammed AliNoch keine Bewertungen
- COSHH Sodium MetabisulfiteDokument3 SeitenCOSHH Sodium MetabisulfiteAhmad OmarNoch keine Bewertungen
- Safety Bulletin - Accdient During Ladder Cutting OperationDokument2 SeitenSafety Bulletin - Accdient During Ladder Cutting OperationalberioNoch keine Bewertungen
- Piper Alpha IncidentDokument31 SeitenPiper Alpha IncidentKhairul ZakirinNoch keine Bewertungen
- Safety ProgramDokument21 SeitenSafety ProgramSits RdddNoch keine Bewertungen
- ABC Oilfield Services Emergency Drill RecordDokument1 SeiteABC Oilfield Services Emergency Drill RecordJaijeev PaliNoch keine Bewertungen
- 01-Ppe Eng PDFDokument17 Seiten01-Ppe Eng PDFZaki AdamouNoch keine Bewertungen
- Book NEBOSH Course in Islamabad PakistanDokument3 SeitenBook NEBOSH Course in Islamabad PakistanHaseebNoch keine Bewertungen
- BP Safety AlertDokument2 SeitenBP Safety AlertRikza AhmadNoch keine Bewertungen
- Ventilation Plan TemplateDokument11 SeitenVentilation Plan TemplatePlank89Noch keine Bewertungen
- Hot Work Procedure 2021Dokument8 SeitenHot Work Procedure 2021Wan Ahmad FaaizunNoch keine Bewertungen
- Types of HazardsDokument2 SeitenTypes of HazardsRosalie Tilos OritoNoch keine Bewertungen
- PSCEMENT PACKER SAFETYDokument2 SeitenPSCEMENT PACKER SAFETYaneshseNoch keine Bewertungen
- 4 Steps To Spill Response: Prevention: The Best SolutionDokument4 Seiten4 Steps To Spill Response: Prevention: The Best SolutionJuan Carlos Guerrero RNoch keine Bewertungen
- Lead Awareness Toolbox TalkDokument2 SeitenLead Awareness Toolbox Talkarunengg100% (1)
- Hot Work Program PDFDokument49 SeitenHot Work Program PDFAnonymous wtK1AZBiNoch keine Bewertungen
- Check Hard Hat Expiry Dates Before UseDokument1 SeiteCheck Hard Hat Expiry Dates Before UsetimbulNoch keine Bewertungen
- BP/ISS Safety Moment - Focusing on the Golden RulesDokument7 SeitenBP/ISS Safety Moment - Focusing on the Golden RulesChristine RossNoch keine Bewertungen
- Summary Slide: Tutorial 1 Safety Culture & Safety ManagementDokument23 SeitenSummary Slide: Tutorial 1 Safety Culture & Safety ManagementChirag Bhanvadia100% (1)
- MSDS Natural Gas Condensate - SweetDokument10 SeitenMSDS Natural Gas Condensate - SweetMuhammad Naufal Nazhib KhanNoch keine Bewertungen
- Occupational Hazards Water Treatment ProcessesDokument14 SeitenOccupational Hazards Water Treatment ProcessesMohamed Salem100% (1)
- Compressed Gas Cylinders PowerPointDokument20 SeitenCompressed Gas Cylinders PowerPointInspire KharianNoch keine Bewertungen
- HSE Emergency Response ChecklistDokument4 SeitenHSE Emergency Response ChecklistMargaretta WijayantiNoch keine Bewertungen
- Safe Work Practice: Title General Application Protective MechanismsDokument1 SeiteSafe Work Practice: Title General Application Protective MechanismseankiboNoch keine Bewertungen
- Pneumatic Test in Piping IncidentDokument6 SeitenPneumatic Test in Piping Incidentfpfps990Noch keine Bewertungen
- Ethanol Tank Fire Incident ReportDokument20 SeitenEthanol Tank Fire Incident ReportN P Srinivasarao100% (1)
- Qa Imco Hse Ms QT 001 Hse Management SystemDokument21 SeitenQa Imco Hse Ms QT 001 Hse Management SystemFrancis Enriquez TanNoch keine Bewertungen
- Behavior-based safety A Clear and Concise ReferenceVon EverandBehavior-based safety A Clear and Concise ReferenceNoch keine Bewertungen
- Fire-Rescue 59: My Mid-Life Crisis as a Volunteer Firefighter-EMTVon EverandFire-Rescue 59: My Mid-Life Crisis as a Volunteer Firefighter-EMTNoch keine Bewertungen
- Safety Engineer: Passbooks Study GuideVon EverandSafety Engineer: Passbooks Study GuideNoch keine Bewertungen
- Hazardous Substances and Human Health: Exposure, Impact and External Cost Assessment at the European ScaleVon EverandHazardous Substances and Human Health: Exposure, Impact and External Cost Assessment at the European ScaleNoch keine Bewertungen
- Exam For Module123Dokument12 SeitenExam For Module123Kian TecsonNoch keine Bewertungen
- Report #1: Alternating-Current Project: Steam-Electric Power PlantDokument41 SeitenReport #1: Alternating-Current Project: Steam-Electric Power PlantKian TecsonNoch keine Bewertungen
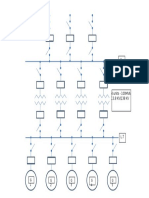
- Single Line DiagramDokument1 SeiteSingle Line DiagramKian TecsonNoch keine Bewertungen
- Formosa Plastics Fire Case Study: Evaluating Process HazardsDokument16 SeitenFormosa Plastics Fire Case Study: Evaluating Process HazardsSaurabh ShahNoch keine Bewertungen
- Table VDDokument1 SeiteTable VDKian TecsonNoch keine Bewertungen
- REPORT#5 Alteranating Current Power PlantDokument9 SeitenREPORT#5 Alteranating Current Power PlantKian TecsonNoch keine Bewertungen
- Program ObjectivesDokument2 SeitenProgram ObjectivesKian TecsonNoch keine Bewertungen
- E-Gizmo Product CatalogDokument219 SeitenE-Gizmo Product CatalogMark BaduaNoch keine Bewertungen
- Lighting Lumen Calculation Sheet SEODokument3 SeitenLighting Lumen Calculation Sheet SEOKian TecsonNoch keine Bewertungen
- Single Phase Outlet ControlDokument17 SeitenSingle Phase Outlet ControlKian TecsonNoch keine Bewertungen
- Thermal Conductivity Thermal ResistanceDokument30 SeitenThermal Conductivity Thermal ResistanceKian TecsonNoch keine Bewertungen
- Illumination Lighitng LevelDokument23 SeitenIllumination Lighitng LevelMandip PokharelNoch keine Bewertungen
- University Floorplan CalculationsDokument789 SeitenUniversity Floorplan CalculationsKian TecsonNoch keine Bewertungen
- Circuit Breaker Interrupting Capacity and Short Time Current RatingsDokument6 SeitenCircuit Breaker Interrupting Capacity and Short Time Current RatingsNagendra PrasadNoch keine Bewertungen
- Spectre - Whitecroft LightingDokument2 SeitenSpectre - Whitecroft LightingKian TecsonNoch keine Bewertungen
- 008 - Electrical Machines II PDFDokument133 Seiten008 - Electrical Machines II PDFaathavan1991Noch keine Bewertungen
- Illumination DesignDokument140 SeitenIllumination DesignKian TecsonNoch keine Bewertungen
- Elective 4 Assignment:: Submitted By: Aldrian Kian B. TecsonDokument5 SeitenElective 4 Assignment:: Submitted By: Aldrian Kian B. TecsonKian TecsonNoch keine Bewertungen
- Code of ProtectionDokument19 SeitenCode of ProtectionMuhammad Altaf KashifNoch keine Bewertungen
- Microprocessor FinalsDokument3 SeitenMicroprocessor FinalsKian TecsonNoch keine Bewertungen
- Motor ParametersDokument2 SeitenMotor Parameterssajs201Noch keine Bewertungen
- 100 Relay DevicesDokument14 Seiten100 Relay DevicesKian TecsonNoch keine Bewertungen
- Electrical Equipment Working Space RequirementsDokument7 SeitenElectrical Equipment Working Space RequirementsKian Tecson100% (5)
- Types of Loudspeaker Baffles ExplainedDokument7 SeitenTypes of Loudspeaker Baffles ExplainedKian TecsonNoch keine Bewertungen
- Gas or Vapor ConstantsDokument5 SeitenGas or Vapor ConstantsKian TecsonNoch keine Bewertungen
- Communications ProjectDokument52 SeitenCommunications ProjectKian TecsonNoch keine Bewertungen
- ANSI Device NumbersDokument7 SeitenANSI Device Numbersrajpre1213Noch keine Bewertungen
- HandoutsDokument2 SeitenHandoutsKian TecsonNoch keine Bewertungen
- Device CodeDokument15 SeitenDevice CodeLakshmanan SivalingamNoch keine Bewertungen
- Nurses' disaster response competencies at health centers in Bireuen District, AcehDokument15 SeitenNurses' disaster response competencies at health centers in Bireuen District, AcehWahyu HidayatiNoch keine Bewertungen
- Rhetorical Analysis of The American Red CrossDokument6 SeitenRhetorical Analysis of The American Red Crossapi-339907931Noch keine Bewertungen
- Fundamentals of Disaster ManagementDokument26 SeitenFundamentals of Disaster ManagementOm KNoch keine Bewertungen
- National Disaster Management Centre: Department of Cooperative Governance and Traditional AffairsDokument20 SeitenNational Disaster Management Centre: Department of Cooperative Governance and Traditional AffairsHerVinaBintiAhmadEl-GubhNoch keine Bewertungen
- Performance Task Family Preparedness Plan W9Dokument5 SeitenPerformance Task Family Preparedness Plan W9Psalm Ezrah LavadoNoch keine Bewertungen
- Monthly Inspection ChecklistDokument3 SeitenMonthly Inspection ChecklistRameeSahibaNoch keine Bewertungen
- Spanish For Dummies Cheat SheetDokument3 SeitenSpanish For Dummies Cheat Sheetjharajnish30Noch keine Bewertungen
- Disaster Continuum: Scaling The Heights of Flexible LearningDokument25 SeitenDisaster Continuum: Scaling The Heights of Flexible LearningKRIZIA ANE A. SULONGNoch keine Bewertungen
- Brockton Police Log 6/7/2019Dokument18 SeitenBrockton Police Log 6/7/2019BBNoch keine Bewertungen
- Disaster NursingDokument14 SeitenDisaster Nursingangelogrande67% (3)
- Ship's Lifeboats - Analysis of Accident Cause and Effect and Its Relationship To Seafarers' Hazard PerceptionDokument153 SeitenShip's Lifeboats - Analysis of Accident Cause and Effect and Its Relationship To Seafarers' Hazard PerceptionScotch_Y100% (1)
- Kuiz BombaDokument2 SeitenKuiz Bombakaren limNoch keine Bewertungen
- School Earthquake DrillDokument22 SeitenSchool Earthquake DrillRozel Laigo Reyes71% (7)
- Blunt Trauma: Vic V. Vernenkar, D.O. St. Barnabas Hospital Dept. of SurgeryDokument87 SeitenBlunt Trauma: Vic V. Vernenkar, D.O. St. Barnabas Hospital Dept. of SurgeryGersonito SobreiraNoch keine Bewertungen
- National Service Reserve Corps: Eillen B. Villamera NSTP FacilitatorDokument33 SeitenNational Service Reserve Corps: Eillen B. Villamera NSTP FacilitatorANJEANETH MENDEZNoch keine Bewertungen
- Crisis Management Manual Manual 1996Dokument62 SeitenCrisis Management Manual Manual 1996jomar ico100% (1)
- Making An Evacuation Plan 3Dokument49 SeitenMaking An Evacuation Plan 3FG Summer100% (1)
- Global Maritime Distress and Safety System CourseDokument13 SeitenGlobal Maritime Distress and Safety System Coursecatalin100% (2)
- Emergency ResponseDokument5 SeitenEmergency ResponseSepeta Sululu OlesaunaNoch keine Bewertungen
- FM 19-10 Military Police Law and Order OperationsDokument235 SeitenFM 19-10 Military Police Law and Order OperationsMark Cheney100% (1)
- 2012 DILG Region 02 Annual Report Highlights Key Programs and InitiativesDokument39 Seiten2012 DILG Region 02 Annual Report Highlights Key Programs and InitiativesVilma Baltazar Aganus100% (1)
- Earthquake Family PreparednessDokument9 SeitenEarthquake Family PreparednessirecNoch keine Bewertungen
- Disaster Preparedness in BDDokument36 SeitenDisaster Preparedness in BDMohib ShamimNoch keine Bewertungen
- Santa Barbara County Thomas Fire and Montecito Debris Flow After Action Report and Improvement PlanDokument36 SeitenSanta Barbara County Thomas Fire and Montecito Debris Flow After Action Report and Improvement Plangiana_magnoliNoch keine Bewertungen
- Aberrant d20 PDFDokument234 SeitenAberrant d20 PDFlolcityNoch keine Bewertungen
- Financial Services Authority BCM GuideDokument38 SeitenFinancial Services Authority BCM Guiderobb35mmNoch keine Bewertungen
- Interview QuestionDokument2 SeitenInterview Questionmarikarthi100% (1)
- UCO Operations 2017, UCO Reporter, October Edition, September 29, 2017Dokument60 SeitenUCO Operations 2017, UCO Reporter, October Edition, September 29, 2017ucopresident_2130533Noch keine Bewertungen
- Emergency Evacuation of Offshore InstallationDokument15 SeitenEmergency Evacuation of Offshore Installationidhur61Noch keine Bewertungen
- Hexayurt Design Like You Give A DamnDokument4 SeitenHexayurt Design Like You Give A DamnBURNcastNoch keine Bewertungen