Das könnte Ihnen auch gefallen
- Case Report - Juliet - Closed Fracture Middle of The Left FemurDokument28 SeitenCase Report - Juliet - Closed Fracture Middle of The Left FemurGupiesNoch keine Bewertungen
- Open Fracture 1/3 Middle Femur Sinistra: Case ReportDokument30 SeitenOpen Fracture 1/3 Middle Femur Sinistra: Case ReportAnggita Efipania Silambi'Noch keine Bewertungen
- Closed Fracture TibialDokument41 SeitenClosed Fracture TibiallukitaniningNoch keine Bewertungen
- Case ReportDokument32 SeitenCase Reportsul11Noch keine Bewertungen
- Closed Fraktur Distal Tibia FibulaDokument27 SeitenClosed Fraktur Distal Tibia FibulaAnggita Efipania Silambi'Noch keine Bewertungen
- CBD-Fracture of Shaft FemurDokument34 SeitenCBD-Fracture of Shaft FemurBONG AIKCHINGNoch keine Bewertungen
- Ortho Fraktur 1/3 Proximal Humerus DextraDokument57 SeitenOrtho Fraktur 1/3 Proximal Humerus DextraFian ChristoNoch keine Bewertungen
- Case ReportDokument29 SeitenCase ReportMagnusNoch keine Bewertungen
- Closed Fracture HumerusDokument35 SeitenClosed Fracture HumerusFloreanHartungiLotisnaNoch keine Bewertungen
- Case Report (Ola)Dokument44 SeitenCase Report (Ola)amel015Noch keine Bewertungen
- Femur Shaft Fracture PresentationDokument27 SeitenFemur Shaft Fracture PresentationZulkarnain HasyimNoch keine Bewertungen
- Case Report Juli 2013Dokument21 SeitenCase Report Juli 2013NahdiaNoch keine Bewertungen
- Fractures HFHDokument74 SeitenFractures HFHEmmanuel Papa AcquahNoch keine Bewertungen
- Closed Segmental Fracture Left Tibia Closed Fracture 1/3 Middle Left FibulaDokument39 SeitenClosed Segmental Fracture Left Tibia Closed Fracture 1/3 Middle Left FibulaimaNoch keine Bewertungen
- Treating a Closed Supracondylar Fracture of the Right FemurDokument37 SeitenTreating a Closed Supracondylar Fracture of the Right FemurSri Mahtufa Riski100% (1)
- Trauma - Intertrochanteric Fracture - RustiniDokument7 SeitenTrauma - Intertrochanteric Fracture - Rustinidedyalkarni08Noch keine Bewertungen
- CLOSED FRACTURE OF LEFT TIBIAL PLATEAU SCHATZKER VIDokument41 SeitenCLOSED FRACTURE OF LEFT TIBIAL PLATEAU SCHATZKER VIlukitaniningNoch keine Bewertungen
- Open Fracture Tibia Fibula FixDokument42 SeitenOpen Fracture Tibia Fibula Fixannisaoktoviani100% (1)
- Fractures of Forearm: Oktya Veny Simbolon Pattiyah Prehandini AyuningtyasDokument90 SeitenFractures of Forearm: Oktya Veny Simbolon Pattiyah Prehandini AyuningtyaspattiyahNoch keine Bewertungen
- Humeral Fracture TreatmentDokument49 SeitenHumeral Fracture TreatmentIcha Marissa SofyanNoch keine Bewertungen
- Closed Tibia and Fibula Fracture Case PresentationDokument30 SeitenClosed Tibia and Fibula Fracture Case Presentationzhafran_darwisNoch keine Bewertungen
- Elbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsDokument57 SeitenElbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsHajar AlSaediNoch keine Bewertungen
- Immobilization and Transport On Patient FractureDokument58 SeitenImmobilization and Transport On Patient FractureDinaNoch keine Bewertungen
- Pengayaan Koass Ortho - Update 5 VersionDokument122 SeitenPengayaan Koass Ortho - Update 5 Versionanon_967171484Noch keine Bewertungen
- Departement of Orthopaedic and TraumatologyDokument89 SeitenDepartement of Orthopaedic and TraumatologyMukhizalNoch keine Bewertungen
- Femoral Neck FractureDokument28 SeitenFemoral Neck FractureayuegpNoch keine Bewertungen
- Skeletal Trauma-Plain Film Trauma Terminology ReviewDokument35 SeitenSkeletal Trauma-Plain Film Trauma Terminology Reviewbjpalmer100% (3)
- Dr. Yohannes Toban Dr. Michael BenjaminDokument27 SeitenDr. Yohannes Toban Dr. Michael BenjaminFatimah OthmanNoch keine Bewertungen
- Principles Fracture ManagementDokument88 SeitenPrinciples Fracture ManagementYauffa Hanna Elt MisykahNoch keine Bewertungen
- Clavicle FractureDokument15 SeitenClavicle Fracturesalsabil aurellNoch keine Bewertungen
- Case Presentation: HistoryDokument45 SeitenCase Presentation: HistorySaya MenangNoch keine Bewertungen
- Severe Pain and Swelling in Left Leg After Traffic AccidentDokument37 SeitenSevere Pain and Swelling in Left Leg After Traffic AccidentAde Cahyo IslamiNoch keine Bewertungen
- Maxillofacial Trauma: Mandibular Fracture Causes and TreatmentDokument34 SeitenMaxillofacial Trauma: Mandibular Fracture Causes and TreatmentHanin AbukhiaraNoch keine Bewertungen
- All of Surgery IDokument75 SeitenAll of Surgery IAli MjadleNoch keine Bewertungen
- Orthopedic Trauma Office Management of MDokument28 SeitenOrthopedic Trauma Office Management of MVladislav KotovNoch keine Bewertungen
- Surgical Treatment of Neglected Malunion of Shaft Femur: Case ReportDokument13 SeitenSurgical Treatment of Neglected Malunion of Shaft Femur: Case ReportNando OktariNoch keine Bewertungen
- Atls Chapter 8 Musculoskeletal TraumaDokument35 SeitenAtls Chapter 8 Musculoskeletal TraumaPamorNoch keine Bewertungen
- Musculo-Skeletal TraumaDokument48 SeitenMusculo-Skeletal TraumaNagashree VNoch keine Bewertungen
- Blue Writing Is What I Added To These Notes: RadiographyDokument46 SeitenBlue Writing Is What I Added To These Notes: Radiographybjpalmer100% (2)
- Pelvic Fractures: Part 1. Evaluation, Classification, and ResuscitationDokument28 SeitenPelvic Fractures: Part 1. Evaluation, Classification, and ResuscitationRiven OktavianNoch keine Bewertungen
- Chapter 29Dokument93 SeitenChapter 29api-3743202Noch keine Bewertungen
- Diagnostic Imaging - 5 - Fractures-Subluxation-Dislocations - Prof - Dr.İsmet TAMERDokument33 SeitenDiagnostic Imaging - 5 - Fractures-Subluxation-Dislocations - Prof - Dr.İsmet TAMERAly MssreNoch keine Bewertungen
- Orthopedic RSUD Panembahan Senopati BantulDokument28 SeitenOrthopedic RSUD Panembahan Senopati Bantulwinda alviraNoch keine Bewertungen
- 1 Ulnar Radial FX CWU Deirdre%27sDokument7 Seiten1 Ulnar Radial FX CWU Deirdre%27sAyeshaNoch keine Bewertungen
- Fraktur Distal HumerusDokument32 SeitenFraktur Distal HumerussyaifularisNoch keine Bewertungen
- Fracture Dan Penanganan EmergencyDokument52 SeitenFracture Dan Penanganan Emergencyshindie lethulurNoch keine Bewertungen
- FractureDokument125 SeitenFractureKlara Devina VanessaNoch keine Bewertungen
- Fraktur Dan DislokasiDokument77 SeitenFraktur Dan DislokasiRicky Jawwa0% (1)
- P and o SelfDokument443 SeitenP and o SelfDeepa SeiraNoch keine Bewertungen
- Formearm FracturesDokument24 SeitenFormearm FracturesNgô Duy LongNoch keine Bewertungen
- Dr. Arnadi Fraktur & DislokasiDokument77 SeitenDr. Arnadi Fraktur & DislokasiPuji Yunisyah RahayuNoch keine Bewertungen
- Guide to Femoral Shaft and Distal Femur FracturesDokument40 SeitenGuide to Femoral Shaft and Distal Femur FracturesOlasinde AnthonyNoch keine Bewertungen
- Critical Thinking Exercise 4Dokument2 SeitenCritical Thinking Exercise 4SandeepNoch keine Bewertungen
- Tibia Fibula Fanny - 2Dokument27 SeitenTibia Fibula Fanny - 2Rakyat Kecil BerdasiNoch keine Bewertungen
- OA - Ahmad Aulia Rizaly - DR Andry Usman SpOTDokument34 SeitenOA - Ahmad Aulia Rizaly - DR Andry Usman SpOTNur Syamsiah MNoch keine Bewertungen
- Untitled PresentationDokument44 SeitenUntitled PresentationMika PamulangNoch keine Bewertungen
- Femur Shaft FractureDokument33 SeitenFemur Shaft FractureAkash KoulNoch keine Bewertungen
- New Introduction To Ortho 1 Jan 20016Dokument67 SeitenNew Introduction To Ortho 1 Jan 20016BIOLOGY BY ISMAIL ANSARINoch keine Bewertungen
- Distal Clavicle Osteolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandDistal Clavicle Osteolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Diagnosis PrenatalDokument24 SeitenDiagnosis PrenatalmasyfuqNoch keine Bewertungen
- Kegawatdaruratan InternaDokument1 SeiteKegawatdaruratan InternaraniNoch keine Bewertungen
- Bukupedomanpengobatandasardipuskesmasthn2007Dokument1 SeiteBukupedomanpengobatandasardipuskesmasthn2007raniNoch keine Bewertungen
- Rcse9101 002Dokument6 SeitenRcse9101 002Syaoran AuliaNoch keine Bewertungen
- Shoulder Impingement Syndrome: Michael C. Koester, MD, Michael S. George, MD, John E. Kuhn, MDDokument4 SeitenShoulder Impingement Syndrome: Michael C. Koester, MD, Michael S. George, MD, John E. Kuhn, MDraniNoch keine Bewertungen
- StrabismusDokument56 SeitenStrabismusraniNoch keine Bewertungen
- Clinical Examination of The KneeDokument6 SeitenClinical Examination of The KneeraniNoch keine Bewertungen
- Dislokasi Lensa dan Traumatik GlaukomaDokument22 SeitenDislokasi Lensa dan Traumatik GlaukomaraniNoch keine Bewertungen
- Comprehensive guide to knee special testsDokument7 SeitenComprehensive guide to knee special testsraniNoch keine Bewertungen
- Initial Assesment and ManagementDokument48 SeitenInitial Assesment and Managementiqbal743Noch keine Bewertungen
- Ahmed 2022Dokument20 SeitenAhmed 2022Mariela Estefanía Marín LópezNoch keine Bewertungen
- Lesson Plan 2aDokument5 SeitenLesson Plan 2aapi-332424736Noch keine Bewertungen
- Barrett Firearms - REC10 - Operators Manual 8.5x5.5 ALL REVB 17278Dokument22 SeitenBarrett Firearms - REC10 - Operators Manual 8.5x5.5 ALL REVB 17278Ricardo C TorresNoch keine Bewertungen
- GRT9165 Product GuideDokument23 SeitenGRT9165 Product GuideEslamAldenAbdoNoch keine Bewertungen
- DVRP Newsletter Resilience Vol. 2, Issue 2Dokument6 SeitenDVRP Newsletter Resilience Vol. 2, Issue 2Lucius Doxerie Sr.Noch keine Bewertungen
- AR M205 BrochureDokument4 SeitenAR M205 BrochurenickypanzeNoch keine Bewertungen
- GMSARN Conf: Design Criteria on Substation ProtectionDokument6 SeitenGMSARN Conf: Design Criteria on Substation Protectionbdaminda6701Noch keine Bewertungen
- Compression Molding of Gypsum Blocks Using Ecological Brick MachinesDokument11 SeitenCompression Molding of Gypsum Blocks Using Ecological Brick Machinessami fanuaelNoch keine Bewertungen
- Rom BlonDokument8 SeitenRom BlonCharlesJustin AyunonNoch keine Bewertungen
- Ajhgaa English O6Dokument28 SeitenAjhgaa English O6dhirumeshkumarNoch keine Bewertungen
- Casa Cook ArvindDokument65 SeitenCasa Cook ArvindLEAN MauritiusNoch keine Bewertungen
- Presentation 1Dokument26 SeitenPresentation 1Vaibhav Hireraddi100% (1)
- 2G - 4G Network Module - Data Sheet - EnglishDokument8 Seiten2G - 4G Network Module - Data Sheet - EnglishbbwroNoch keine Bewertungen
- Solving Problems Involving Kinds of Propotion StudentDokument18 SeitenSolving Problems Involving Kinds of Propotion StudentJohn Daniel BerdosNoch keine Bewertungen
- 1625-De Dwks Parts ListDokument69 Seiten1625-De Dwks Parts ListSasan AbbasiNoch keine Bewertungen
- Assignment 1 Systems Analysis - EME5601Dokument7 SeitenAssignment 1 Systems Analysis - EME5601Travis GrantNoch keine Bewertungen
- Final 401Dokument8 SeitenFinal 401Hong Chul NamNoch keine Bewertungen
- Got 1000 Connect To Alpha 2Dokument42 SeitenGot 1000 Connect To Alpha 2supriyo110Noch keine Bewertungen
- 02 - AFT - Know Your Pump & System Curves - Part 2ADokument8 Seiten02 - AFT - Know Your Pump & System Curves - Part 2AAlfonso José García LagunaNoch keine Bewertungen
- TDS - RheoFIT 762Dokument2 SeitenTDS - RheoFIT 762Alexi ALfred H. TagoNoch keine Bewertungen
- SmogDokument5 SeitenSmogAlain MoratallaNoch keine Bewertungen
- Lab 7 Activities Sheet Winter 2020Dokument7 SeitenLab 7 Activities Sheet Winter 2020Mareline MendietaNoch keine Bewertungen
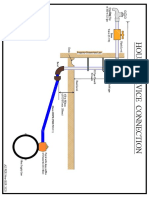
- House Service Connection NEW BSR 2020-1Dokument1 SeiteHouse Service Connection NEW BSR 2020-1Deshraj BairwaNoch keine Bewertungen
- The Indonesian Food Processing Industry (Final)Dokument48 SeitenThe Indonesian Food Processing Industry (Final)patalnoNoch keine Bewertungen
- Tabel Benkelman Beam Baru - AsisDokument21 SeitenTabel Benkelman Beam Baru - AsisAsisNoch keine Bewertungen
- English 6 Action Research Contextualized Materials ProposalDokument41 SeitenEnglish 6 Action Research Contextualized Materials ProposalJake YaoNoch keine Bewertungen
- Actividad 3.1B-Xport-Model-Exercises-SCMDokument5 SeitenActividad 3.1B-Xport-Model-Exercises-SCMDante Rivera SalinasNoch keine Bewertungen
- Comparing characteristics and properties of various crude oilsDokument2 SeitenComparing characteristics and properties of various crude oilsnishant bhushanNoch keine Bewertungen
- Epson LQ-2090Dokument248 SeitenEpson LQ-2090Dejan StamenovNoch keine Bewertungen
- Ring OnlyDokument2 SeitenRing Onlyapi-3834777Noch keine Bewertungen