Das könnte Ihnen auch gefallen
- IM Shelf - AmbossDokument61 SeitenIM Shelf - AmbossHaadi AliNoch keine Bewertungen
- Nursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideVon EverandNursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideNoch keine Bewertungen
- Notes: Heparin-Induced Thrombocytopenia (Hit)Dokument6 SeitenNotes: Heparin-Induced Thrombocytopenia (Hit)MOHIT SHARMANoch keine Bewertungen
- NBME 7 - Answers & Explanations (SP)Dokument70 SeitenNBME 7 - Answers & Explanations (SP)JUAN CHAVEZNoch keine Bewertungen
- Thrombocytopenia Thrombocytopenia Thrombocytopenia ThrombocytopeniaDokument12 SeitenThrombocytopenia Thrombocytopenia Thrombocytopenia ThrombocytopeniaRashed ShatnawiNoch keine Bewertungen
- Hematology AtlasDokument733 SeitenHematology Atlasrakshit09100% (10)
- Hematologic Pathology p1-23Dokument23 SeitenHematologic Pathology p1-23zeroun24100% (2)
- DR Nilukshi Perera Consultant HaematologistDokument68 SeitenDR Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteNoch keine Bewertungen
- PolycythemiaDokument82 SeitenPolycythemiaTiffany Mae Arud100% (3)
- Massive Transfusion章宏吉Dokument48 SeitenMassive Transfusion章宏吉lawlietNoch keine Bewertungen
- Pathology Bleeding DisordersDokument67 SeitenPathology Bleeding DisordersMarcelliaNoch keine Bewertungen
- 15 - Toronto Notes 2011 - HematologyDokument58 Seiten15 - Toronto Notes 2011 - HematologyWaiwit Chotchawjaru100% (1)
- Hematology MCCQE ReviewDokument46 SeitenHematology MCCQE ReviewMustafa Khandgawi100% (1)
- S0850alug 1670953860959-SEU HDokument56 SeitenS0850alug 1670953860959-SEU HAziz KhwajaNoch keine Bewertungen
- Med Surg Chapters 19 - 20 Hematologic Functions and Disorders PPT and QuestionsDokument36 SeitenMed Surg Chapters 19 - 20 Hematologic Functions and Disorders PPT and QuestionsAshley100% (1)
- Disorders of PlateletsfDokument51 SeitenDisorders of PlateletsfSyarifah Tridani FitriaNoch keine Bewertungen
- Week 7. Renal Pathology Continued.Dokument9 SeitenWeek 7. Renal Pathology Continued.Amber LeJeuneNoch keine Bewertungen
- ThrombocytopeniaDokument19 SeitenThrombocytopeniaChiyaanVikram100% (1)
- 6th March 2020 Plab 1 MockDokument32 Seiten6th March 2020 Plab 1 MockZoha QureshiNoch keine Bewertungen
- Diseases of PlateletsDokument86 SeitenDiseases of Plateletsdesktop dolakhaNoch keine Bewertungen
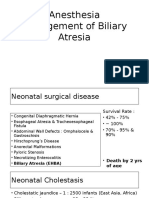
- 19 Anesthesia For Biliary AtresiaDokument19 Seiten19 Anesthesia For Biliary AtresiaDwiki Surya PrayogaNoch keine Bewertungen
- Fast Facts: Leukemia: From initial gene mutation to survivorship supportVon EverandFast Facts: Leukemia: From initial gene mutation to survivorship supportNoch keine Bewertungen
- Bleeding and Coagulation Disorders: DR Nidhi Chaurasia JR-1 MDS PedodonticsDokument66 SeitenBleeding and Coagulation Disorders: DR Nidhi Chaurasia JR-1 MDS PedodonticsDrNidhi KrishnaNoch keine Bewertungen
- Disorder of PlateletsDokument27 SeitenDisorder of PlateletsRoby KieranNoch keine Bewertungen
- Thrombocytopenia: Decreased Production Increased Destruction Sequestration PseudothrombocytopeniaDokument43 SeitenThrombocytopenia: Decreased Production Increased Destruction Sequestration PseudothrombocytopeniaDea Tasha MeicitaNoch keine Bewertungen
- 2007 Nov 07 CompleteDokument62 Seiten2007 Nov 07 CompleteKay BristolNoch keine Bewertungen
- The Spleen: Schwartz's Principles of Surgery 11th EdDokument54 SeitenThe Spleen: Schwartz's Principles of Surgery 11th EdaddelinsNoch keine Bewertungen
- The Spleen: Schwartz's Principles of Surgery 11th EdDokument54 SeitenThe Spleen: Schwartz's Principles of Surgery 11th EdMuhammad Fhandeka IsrarNoch keine Bewertungen
- MyeloproliferativeDokument9 SeitenMyeloproliferativeRashed ShatnawiNoch keine Bewertungen
- Causes of Thromboctyopenia &Dokument30 SeitenCauses of Thromboctyopenia &Rishabh SinghNoch keine Bewertungen
- 116 - Disorders of HemostasisDokument13 Seiten116 - Disorders of HemostasisMuliyamanNoch keine Bewertungen
- Week 14 PLT DisorderDokument74 SeitenWeek 14 PLT Disorderiamtrcmrvr922Noch keine Bewertungen
- ThrombocytopeniaDokument9 SeitenThrombocytopeniaamjad_muslehNoch keine Bewertungen
- ThrombocytopeniaDokument3 SeitenThrombocytopeniaSara Abdi OsmanNoch keine Bewertungen
- Case DiscussionDokument29 SeitenCase DiscussionRachmad Ricky ArnandyNoch keine Bewertungen
- Why Does My Patient Have Thrombocytopenia PDFDokument22 SeitenWhy Does My Patient Have Thrombocytopenia PDFElena Villarreal100% (1)
- Thrombocytopenia Thrombotic Thrombocytopenic Purpura: DR Ahmad Abu Al-Samen MDDokument17 SeitenThrombocytopenia Thrombotic Thrombocytopenic Purpura: DR Ahmad Abu Al-Samen MDmohNoch keine Bewertungen
- Approach To Febrile Thrombocytopenia by SudeshDokument20 SeitenApproach To Febrile Thrombocytopenia by Sudeshkkmbbsdnb100% (1)
- 1 s2.0 S0899588513000701 Main PDFDokument8 Seiten1 s2.0 S0899588513000701 Main PDFRicki HanNoch keine Bewertungen
- PRESENTED:-Dr. Raju NiraulaDokument29 SeitenPRESENTED:-Dr. Raju NiraulaRaju NiraulaNoch keine Bewertungen
- Thrombocytopenia: What We Will Cover TodayDokument23 SeitenThrombocytopenia: What We Will Cover TodayKimbek BuangkeNoch keine Bewertungen
- Thrombotic Thrombocytopenic Purpura PDFDokument6 SeitenThrombotic Thrombocytopenic Purpura PDFDany EdyNoch keine Bewertungen
- ET (New), UMI Juli 2013Dokument15 SeitenET (New), UMI Juli 2013L M AkhiruddinNoch keine Bewertungen
- 2014 - Trombotic MicroangiopathiesDokument23 Seiten2014 - Trombotic MicroangiopathiesLuis Fernando Morales JuradoNoch keine Bewertungen
- Platelet: Muhammad Nazarudin, S.STDokument15 SeitenPlatelet: Muhammad Nazarudin, S.STFafha FafhaNoch keine Bewertungen
- 2013 GuthMay8 SplenectomyDokument24 Seiten2013 GuthMay8 SplenectomyKNoch keine Bewertungen
- An Approach To Bleeding DisordersDokument30 SeitenAn Approach To Bleeding DisordersSiddique BhattiNoch keine Bewertungen
- Trombositopenia Dan TrombositosisDokument33 SeitenTrombositopenia Dan TrombositosisAim AimmaNoch keine Bewertungen
- Idiopathic Thrombocytopenic PurpuraDokument5 SeitenIdiopathic Thrombocytopenic Purpurasaputra tri nopiantoNoch keine Bewertungen
- Polycythemia: Pearla LasutDokument22 SeitenPolycythemia: Pearla LasutFuji YantoNoch keine Bewertungen
- Lecture 3. Bleeding Disorders Part 1Dokument31 SeitenLecture 3. Bleeding Disorders Part 1Kekelwa Mutumwenu Snr100% (1)
- Thrombocytopenia in The Intensive Care UnitDokument35 SeitenThrombocytopenia in The Intensive Care UnitMarcelliaNoch keine Bewertungen
- 10.21.09 Jenkins TTPDokument16 Seiten10.21.09 Jenkins TTPOdiliaDeaNovenaNoch keine Bewertungen
- Lecture 16 - Bleeding Tendency DiseasesDokument64 SeitenLecture 16 - Bleeding Tendency Diseasesapi-3703352100% (1)
- Polycythemia: Lecture Slides Pratap Sagar Tiwari, MDDokument17 SeitenPolycythemia: Lecture Slides Pratap Sagar Tiwari, MDYan PetrovNoch keine Bewertungen
- Thrombotic Thrombocytopenic PurpuraDokument5 SeitenThrombotic Thrombocytopenic PurpuraAhsan Tanio DaulayNoch keine Bewertungen
- Case Discussion: Huang Honghui Department of Hematology Ren Ji HospitalDokument29 SeitenCase Discussion: Huang Honghui Department of Hematology Ren Ji HospitalronaldsacsNoch keine Bewertungen
- Complete Blood CountDokument18 SeitenComplete Blood CountNazih MominNoch keine Bewertungen
- ThrombocytopeniaDokument4 SeitenThrombocytopeniaValerrie NgenoNoch keine Bewertungen
- Idiopathic Thrombocytopenic Purpura: Bruising Petechiae Nosebleeds GumsDokument7 SeitenIdiopathic Thrombocytopenic Purpura: Bruising Petechiae Nosebleeds GumsMahirina Marjani ZulkifliNoch keine Bewertungen
- The SpleenDokument53 SeitenThe SpleenfayazNoch keine Bewertungen
- Idiopathic Thrombocytopenic PurpuraDokument11 SeitenIdiopathic Thrombocytopenic PurpuraMelDred Cajes BolandoNoch keine Bewertungen
- Hematopoiesis Is The Complex Process of The Formation and Maturation of Blood CellsDokument35 SeitenHematopoiesis Is The Complex Process of The Formation and Maturation of Blood CellsYary MayorNoch keine Bewertungen
- DR Prakash Nag MD Medicine NGMCDokument70 SeitenDR Prakash Nag MD Medicine NGMCSamjhana NeupaneNoch keine Bewertungen
- VND Openxmlformats-Officedocument Presentationml Presentation&rendition 1-9Dokument25 SeitenVND Openxmlformats-Officedocument Presentationml Presentation&rendition 1-9Abdul Gafoor CPNoch keine Bewertungen
- Bone Marrow Failure 2008-09Dokument15 SeitenBone Marrow Failure 2008-09Karan BhattNoch keine Bewertungen
- Polycythemia Rubra VeraDokument10 SeitenPolycythemia Rubra VeraMardhiyyah MazlanNoch keine Bewertungen
- Bleeding Disorders in Pregnancy: Table 1Dokument7 SeitenBleeding Disorders in Pregnancy: Table 1KharismaNisaNoch keine Bewertungen
- Hematology: Jan Bazner-Chandler CPNP, CNS, MSN, RNDokument80 SeitenHematology: Jan Bazner-Chandler CPNP, CNS, MSN, RNWarrenPeaceNoch keine Bewertungen
- 9 Rinawati Batam 11 Sept - PerioperativDokument57 Seiten9 Rinawati Batam 11 Sept - PerioperativDwiki Surya PrayogaNoch keine Bewertungen
- Greeting From Korea KLMPKDokument8 SeitenGreeting From Korea KLMPKDwiki Surya PrayogaNoch keine Bewertungen
- Thrombocytos Is: DR Putra Hendra SPPD UnibaDokument22 SeitenThrombocytos Is: DR Putra Hendra SPPD UnibaDwiki Surya PrayogaNoch keine Bewertungen
- Lymphadenopathy Uniba 18-1-13Dokument34 SeitenLymphadenopathy Uniba 18-1-13Dwiki Surya PrayogaNoch keine Bewertungen
- 4 Early Diagnosis in Neonatal Surgical CasesDokument64 Seiten4 Early Diagnosis in Neonatal Surgical CasesDwiki Surya PrayogaNoch keine Bewertungen
- Hemolytic Anemia - Evaluation and Differential DiagnosisDokument11 SeitenHemolytic Anemia - Evaluation and Differential DiagnosisfrenteNoch keine Bewertungen
- Muhammad Asif Zeb Lecturer Hematology Ipms-KmuDokument21 SeitenMuhammad Asif Zeb Lecturer Hematology Ipms-KmuHanif ullahNoch keine Bewertungen
- Group 7 Case StudyDokument4 SeitenGroup 7 Case StudyROSE GARETH SEGYEPNoch keine Bewertungen
- Vascular DiseasesDokument9 SeitenVascular DiseasesJose SirittNoch keine Bewertungen
- Dangerous Conditions WheelDokument4 SeitenDangerous Conditions WheelAdam AdamakoNoch keine Bewertungen
- Directives Blood and Components RwandaDokument68 SeitenDirectives Blood and Components RwandaOLIVIERNoch keine Bewertungen
- Hemolytic Uremic Syndrome: Doyeun OhDokument51 SeitenHemolytic Uremic Syndrome: Doyeun OhMarcelliaNoch keine Bewertungen
- Hematology UQU 2022Dokument94 SeitenHematology UQU 2022Elyas MehdarNoch keine Bewertungen
- By: DR Najibullah Suhraby FMR First YearDokument33 SeitenBy: DR Najibullah Suhraby FMR First YearShami PokhrelNoch keine Bewertungen
- Blood Products and Their UsesDokument28 SeitenBlood Products and Their UsesJeevitha Vanitha100% (1)
- HemaDokument17 SeitenHemakamaluNoch keine Bewertungen
- Icsh Hemostasis Critical ValuesDokument12 SeitenIcsh Hemostasis Critical Valuescitometria prolabNoch keine Bewertungen
- CBE - Platelet AbnormalitiesDokument3 SeitenCBE - Platelet AbnormalitiesRuxandra MesarosNoch keine Bewertungen
- Etiology and Management of Postpartum Hypertension-PreeclampsiaDokument6 SeitenEtiology and Management of Postpartum Hypertension-Preeclampsiawilliamjhon57Noch keine Bewertungen
- Itp TTP Pic DXNDokument4 SeitenItp TTP Pic DXNmaryminNoch keine Bewertungen
- Congenital and Aquired Hemolytic Anemias QuestionsDokument36 SeitenCongenital and Aquired Hemolytic Anemias QuestionstoniassafNoch keine Bewertungen
- De Novo Thrombotic Microangiopathy After Kidney TransplantationDokument11 SeitenDe Novo Thrombotic Microangiopathy After Kidney TransplantationYaxkin NikNoch keine Bewertungen
- Therapeutic Plasma Exchange (TPE) : Colm Magee, MD, MPH, MRCPIDokument23 SeitenTherapeutic Plasma Exchange (TPE) : Colm Magee, MD, MPH, MRCPIsigitNoch keine Bewertungen
- Thrombocytopenia Thrombotic Thrombocytopenic Purpura: DR Ahmad Abu Al-Samen MDDokument17 SeitenThrombocytopenia Thrombotic Thrombocytopenic Purpura: DR Ahmad Abu Al-Samen MDmohNoch keine Bewertungen
- Thrombocytopenia and Thrombocytosis Thrombocytopenia and ThrombocytosisDokument51 SeitenThrombocytopenia and Thrombocytosis Thrombocytopenia and ThrombocytosisPamela MendozaNoch keine Bewertungen
- Phenomenology of Squalor, Hoarding and Self-NeglectDokument5 SeitenPhenomenology of Squalor, Hoarding and Self-NeglectastrogliaNoch keine Bewertungen
- Haematology LastDokument65 SeitenHaematology LastficocNoch keine Bewertungen