Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- William S. Breitbart - Meaning-Centered Psychotherapy in The Cancer Setting - Finding Meaning and Hope in The Face of Suffering (2017, Oxford University Press)Dokument425 SeitenWilliam S. Breitbart - Meaning-Centered Psychotherapy in The Cancer Setting - Finding Meaning and Hope in The Face of Suffering (2017, Oxford University Press)Nicole Marie-Madeleine Alberto100% (2)
- SOAP NOTE SinusitisDokument3 SeitenSOAP NOTE SinusitisMaria Ines Ortiz0% (1)
- Refresher Course: Preboard Examination Nursing Practice III: Care of Clients With Physiologic and Psychosocial Alterations (Part A)Dokument9 SeitenRefresher Course: Preboard Examination Nursing Practice III: Care of Clients With Physiologic and Psychosocial Alterations (Part A)Jastine Sabornido0% (1)
- Louis Kuhne - Neo-Naturopathy (New Science of Healing) (1917)Dokument313 SeitenLouis Kuhne - Neo-Naturopathy (New Science of Healing) (1917)Școala Solomonară / The Solomonary School100% (16)
- Homo Gen Itasse Sung Guh NyaDokument15 SeitenHomo Gen Itasse Sung Guh Nyamursidstone.mursidNoch keine Bewertungen
- Radiological Aspect of Respiratory Diseases (Prof. Arif)Dokument33 SeitenRadiological Aspect of Respiratory Diseases (Prof. Arif)mursidstone.mursid100% (1)
- EDIT Respiratory Failure Assessment and Problem SolvingDokument66 SeitenEDIT Respiratory Failure Assessment and Problem Solvingmursidstone.mursidNoch keine Bewertungen
- EDIT Respiratory Failure Assessment and Problem SolvingDokument66 SeitenEDIT Respiratory Failure Assessment and Problem Solvingmursidstone.mursidNoch keine Bewertungen
- The Role of Angiography and Interventional RadiologyDokument26 SeitenThe Role of Angiography and Interventional Radiologymursidstone.mursidNoch keine Bewertungen
- Radiological Aspect of Cardiovascular DiseasesDokument71 SeitenRadiological Aspect of Cardiovascular Diseasesmursidstone.mursidNoch keine Bewertungen
- Approach To Respiratory Tract InfectionDokument51 SeitenApproach To Respiratory Tract Infectionmursidstone.mursidNoch keine Bewertungen
- Approach To Respiratory Tract InfectionDokument51 SeitenApproach To Respiratory Tract Infectionmursidstone.mursidNoch keine Bewertungen
- Circulation and RespirationDokument18 SeitenCirculation and Respirationmursidstone.mursidNoch keine Bewertungen
- Anatomy 2Dokument6 SeitenAnatomy 2mursidstone.mursidNoch keine Bewertungen
- Circulation and RespirationDokument18 SeitenCirculation and Respirationmursidstone.mursidNoch keine Bewertungen
- Management of Gas Exchange DisturbanceDokument38 SeitenManagement of Gas Exchange Disturbancemursidstone.mursidNoch keine Bewertungen
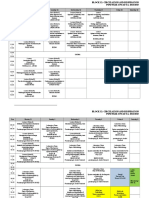
- Revisi Jadwal Blok 12 PK - 2015Dokument7 SeitenRevisi Jadwal Blok 12 PK - 2015mursidstone.mursidNoch keine Bewertungen
- Respiratory SystemDokument18 SeitenRespiratory Systemmursidstone.mursidNoch keine Bewertungen
- CVD Screening PaperDokument4 SeitenCVD Screening Papermursidstone.mursidNoch keine Bewertungen
- Recommendations For The Cardiovascular Screening of AthletesDokument8 SeitenRecommendations For The Cardiovascular Screening of Athletesmursidstone.mursidNoch keine Bewertungen
- Estimation of Maximum Oxygen Uptake by Evaluating Cooper 12-Min Run Test in Female Students of West Bengal, IndiaDokument7 SeitenEstimation of Maximum Oxygen Uptake by Evaluating Cooper 12-Min Run Test in Female Students of West Bengal, Indiamursidstone.mursidNoch keine Bewertungen
- Tutor 3Dokument21 SeitenTutor 3mursidstone.mursidNoch keine Bewertungen
- Pulmonary FX Test PDFDokument7 SeitenPulmonary FX Test PDFmursidstone.mursidNoch keine Bewertungen
- Guidelines CVD PreventionDokument77 SeitenGuidelines CVD PreventionAfdol Triatmojo SikumbangNoch keine Bewertungen
- Daftar Pustaka: Systematic Review. WHO. (Cited 2016 September 03) - Available FromDokument6 SeitenDaftar Pustaka: Systematic Review. WHO. (Cited 2016 September 03) - Available Frommursidstone.mursidNoch keine Bewertungen
- Lampiran 2 Analisis Data Pengujian Distribusi Data: Case Processing SummaryDokument8 SeitenLampiran 2 Analisis Data Pengujian Distribusi Data: Case Processing Summarymursidstone.mursidNoch keine Bewertungen
- Dapus Ucit NewDokument6 SeitenDapus Ucit Newmursidstone.mursidNoch keine Bewertungen
- Aedes Sp. Analysis of Variance Baden Aniline and Soda FactoryDokument3 SeitenAedes Sp. Analysis of Variance Baden Aniline and Soda Factorymursidstone.mursidNoch keine Bewertungen
- Daftar Pustaka: Systematic Review. WHO. (Cited 2016 September 03) - Available FromDokument6 SeitenDaftar Pustaka: Systematic Review. WHO. (Cited 2016 September 03) - Available Frommursidstone.mursidNoch keine Bewertungen
- Aedes Sp. Analysis of Variance Baden Aniline and Soda FactoryDokument3 SeitenAedes Sp. Analysis of Variance Baden Aniline and Soda Factorymursidstone.mursidNoch keine Bewertungen
- Anova Atp Basf Che Adenosine Trifosfat: Analysis of VariansDokument1 SeiteAnova Atp Basf Che Adenosine Trifosfat: Analysis of Variansmursidstone.mursidNoch keine Bewertungen
- Aedes Sp. Analysis of Variance Baden Aniline and Soda FactoryDokument3 SeitenAedes Sp. Analysis of Variance Baden Aniline and Soda Factorymursidstone.mursidNoch keine Bewertungen
- Daftar SingkatanDokument1 SeiteDaftar Singkatanmursidstone.mursidNoch keine Bewertungen
- Aedes Sp. Analysis of Variance Baden Aniline and Soda FactoryDokument3 SeitenAedes Sp. Analysis of Variance Baden Aniline and Soda Factorymursidstone.mursidNoch keine Bewertungen
- Autoimmune Rheumatic DiseasesDokument3 SeitenAutoimmune Rheumatic DiseasesBuat DownloadNoch keine Bewertungen
- HipoglikemiaDokument13 SeitenHipoglikemiaRC Ria Chairul100% (1)
- Cardiac MarkersDokument23 SeitenCardiac Markerssulastri triNoch keine Bewertungen
- Physics With Illustrative Examples From Medicine and BiologyDokument1 SeitePhysics With Illustrative Examples From Medicine and BiologySivaranjaniNoch keine Bewertungen
- Dr. Manella Joseph Senior Lecturer/Consultant PathologistDokument41 SeitenDr. Manella Joseph Senior Lecturer/Consultant PathologistNipun Shamika100% (1)
- Daftar Singkatan SMF JAntungDokument5 SeitenDaftar Singkatan SMF JAntungBobby RahmantoNoch keine Bewertungen
- MycinDokument7 SeitenMycinAnirudh GuptaNoch keine Bewertungen
- Lupus Anticoagulant Profile Testing AlgorithmDokument1 SeiteLupus Anticoagulant Profile Testing Algorithmsalamon2tNoch keine Bewertungen
- Chapter 17 End-Of-Life CareDokument29 SeitenChapter 17 End-Of-Life CarePearl DiBerardinoNoch keine Bewertungen
- Hospital Design - AUHDokument108 SeitenHospital Design - AUHDion LakonawaNoch keine Bewertungen
- Generic Name: BudesonideDokument8 SeitenGeneric Name: BudesonidemeangelmeNoch keine Bewertungen
- Abnormal Urinalysis Children-Tadulako2015Dokument33 SeitenAbnormal Urinalysis Children-Tadulako2015Yeyen Hastriam AkramNoch keine Bewertungen
- Superior Laryngeal Nerve InjuryDokument11 SeitenSuperior Laryngeal Nerve InjuryBrilli Bagus DipoNoch keine Bewertungen
- Unicef: General InformationDokument2 SeitenUnicef: General InformationjobNoch keine Bewertungen
- B Auch Muller 2015Dokument7 SeitenB Auch Muller 2015AdityaNoch keine Bewertungen
- Case Investigation Form Coronavirus Disease (COVID-19) : (Check All That Apply, Refer To Appendix 2)Dokument4 SeitenCase Investigation Form Coronavirus Disease (COVID-19) : (Check All That Apply, Refer To Appendix 2)john dave rougel ManzanoNoch keine Bewertungen
- Helping Psychiatry Residents Cope With Patient SuicideDokument5 SeitenHelping Psychiatry Residents Cope With Patient SuicidedrguillermomedinaNoch keine Bewertungen
- Vol 1 No 1Dokument432 SeitenVol 1 No 1cslee100% (1)
- List of Basic Essential Medicines Ministry of Health Seychelles 2010Dokument14 SeitenList of Basic Essential Medicines Ministry of Health Seychelles 2010portosinNoch keine Bewertungen
- Certificate: of EU Product NotificationDokument2 SeitenCertificate: of EU Product NotificationJsamCondoriNoch keine Bewertungen
- SUPER KIDZ Pain ScaleDokument10 SeitenSUPER KIDZ Pain Scalepfi_jenNoch keine Bewertungen
- United General Hospital ICU Expansion Case StudyDokument7 SeitenUnited General Hospital ICU Expansion Case StudyTeddy Les Holladayz25% (4)
- Report On Januvia DrugDokument10 SeitenReport On Januvia DrugyogenaNoch keine Bewertungen
- Aron FinalDokument70 SeitenAron FinalJaime Pastrana Jr.Noch keine Bewertungen
- Inion Freedom Brochure v2 12-2014Dokument11 SeitenInion Freedom Brochure v2 12-2014Ivo van de KampNoch keine Bewertungen
- Jubilant Life Sciences Research Report PDFDokument50 SeitenJubilant Life Sciences Research Report PDFAbhiroop DasNoch keine Bewertungen