Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
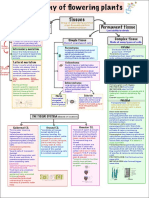
- Anatomy of Flowering Plants Mind MapDokument2 SeitenAnatomy of Flowering Plants Mind MapAstha Agrawal100% (8)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Chicken Wing Dissection InstructionsDokument4 SeitenChicken Wing Dissection InstructionsSandra Fowler100% (1)
- DIGESTIVE Lecture Notes PDFDokument20 SeitenDIGESTIVE Lecture Notes PDFAaliya Minar100% (4)
- Anatomy and Physiology of The AirwayDokument42 SeitenAnatomy and Physiology of The Airwayiaa100% (1)
- S8 - End-of-Unit 1 TestDokument2 SeitenS8 - End-of-Unit 1 TestWilliam Anthony56% (9)
- EB3222 Cell and Tissue Culture: FacultyDokument30 SeitenEB3222 Cell and Tissue Culture: FacultyLeeChiaVuiNoch keine Bewertungen
- ADIL BSN - 1C 11. Manual Reproductive SystemDokument4 SeitenADIL BSN - 1C 11. Manual Reproductive SystemReiko SakaeNoch keine Bewertungen
- The Mechanism of Respiration.Dokument12 SeitenThe Mechanism of Respiration.Shimmering MoonNoch keine Bewertungen
- Amniotic Fluid 2022Dokument40 SeitenAmniotic Fluid 2022Ogbuefi PascalNoch keine Bewertungen
- Ascomycotina Class PPT 2014Dokument80 SeitenAscomycotina Class PPT 2014Shaezarah Mohamudally67% (3)
- The Histopathological Approach To Inflammatory Bowel Disease: A Practice Guide.Dokument18 SeitenThe Histopathological Approach To Inflammatory Bowel Disease: A Practice Guide.Ana CanastraNoch keine Bewertungen
- General Zoology 1 LaboratoryDokument4 SeitenGeneral Zoology 1 LaboratoryKirsten AletheaNoch keine Bewertungen
- Blood Pressure - QuestionsDokument5 SeitenBlood Pressure - QuestionsErjus HoxhajNoch keine Bewertungen
- Call of Cthulhu - 1990 - Delta Green - Handout - Deep One AutopsyDokument2 SeitenCall of Cthulhu - 1990 - Delta Green - Handout - Deep One AutopsyFeartherNoch keine Bewertungen
- Muscular SystemDokument8 SeitenMuscular Systemtheodore_estradaNoch keine Bewertungen
- Integrated Studies Grade 3 Term 1Dokument6 SeitenIntegrated Studies Grade 3 Term 1Kimarley CampbellNoch keine Bewertungen
- MCqs On Hematological Disorder Provided by MirhaDokument4 SeitenMCqs On Hematological Disorder Provided by MirhaAkml KhanNoch keine Bewertungen
- 5 Hemolytic AnemiaDokument72 Seiten5 Hemolytic Anemiacoosa liquorsNoch keine Bewertungen
- Short Note Biology Form 5-Chapter 1 TransportDokument7 SeitenShort Note Biology Form 5-Chapter 1 Transportsalamah_sabri83% (6)
- The Human Immune SystemDokument24 SeitenThe Human Immune Systemmilka berhaneNoch keine Bewertungen
- Syllabus: 1.1.1 E, F, G, H & J: Homework: Revise All From Today For Your Test 1Dokument36 SeitenSyllabus: 1.1.1 E, F, G, H & J: Homework: Revise All From Today For Your Test 1Nusrat'Felix' KhanNoch keine Bewertungen
- Forensic Past PapersDokument11 SeitenForensic Past PapersMedia PilleNoch keine Bewertungen
- Physiological Changes During Pregnancy 2-1Dokument32 SeitenPhysiological Changes During Pregnancy 2-1PATRICK ROSHAN ANoch keine Bewertungen
- A.D. Pearle - Surgical Technique and Anatomic Study of Latissimus Dorsi and Teres Major Transfers (2006)Dokument9 SeitenA.D. Pearle - Surgical Technique and Anatomic Study of Latissimus Dorsi and Teres Major Transfers (2006)João Pedro ZenattoNoch keine Bewertungen
- Vertebrate Systems SummaryDokument29 SeitenVertebrate Systems SummaryHazel Grace Bellen100% (1)
- CBSE Class 11 Biology Chapter 21 Neural Control and Coordination NotesDokument7 SeitenCBSE Class 11 Biology Chapter 21 Neural Control and Coordination NotesShivalgiri Goswami0% (1)
- Cervical CancerDokument30 SeitenCervical Cancerhuhknee100% (1)
- Tarif Harga RADIOLOGI Murni TeguhDokument24 SeitenTarif Harga RADIOLOGI Murni Teguhester silalahiNoch keine Bewertungen
- Ain Shams University - Clinical Pathology Ain ShamsDokument182 SeitenAin Shams University - Clinical Pathology Ain ShamsRowaa SamehNoch keine Bewertungen
- Ap Bio Unit 2 Quick Study CardDokument1 SeiteAp Bio Unit 2 Quick Study CardAbhi ShahNoch keine Bewertungen