Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shangri-La JKT - JDMDokument2 SeitenShangri-La JKT - JDMscribdNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Ways To Improve The Macrovascular Outcomes in Type 2 Diabetes TherapyDokument42 SeitenWays To Improve The Macrovascular Outcomes in Type 2 Diabetes TherapyscribdNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Unmet Need DM Management in Primary Care Seting 280914Dokument62 SeitenUnmet Need DM Management in Primary Care Seting 280914scribdNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- DMcombos JDM2014Dokument5 SeitenDMcombos JDM2014scribdNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Role of Kidney (Unmet Need in T2DM) For Prof SarwonoDokument25 SeitenRole of Kidney (Unmet Need in T2DM) For Prof SarwonoscribdNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Workshop: Case StudyDokument28 SeitenWorkshop: Case StudyscribdNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Survey Obat DM Poli Endokrin (Prof - Sarwono)Dokument8 SeitenSurvey Obat DM Poli Endokrin (Prof - Sarwono)scribdNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- PDCI Core Kit 15 Indications For Referral of Complex PatientsDokument49 SeitenPDCI Core Kit 15 Indications For Referral of Complex PatientsscribdNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Sist - Penelitian ProDokument57 SeitenSist - Penelitian ProscribdNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- Diabetes Care in Indonesia - Role of GLP 1 Analog: Pradana SoewondoDokument58 SeitenDiabetes Care in Indonesia - Role of GLP 1 Analog: Pradana SoewondoscribdNoch keine Bewertungen
- DMCombos JDM2014Dokument160 SeitenDMCombos JDM2014scribdNoch keine Bewertungen
- Current Concepts of Chronic Diabetic ComplicationsDokument4 SeitenCurrent Concepts of Chronic Diabetic ComplicationsscribdNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- From Evidence to Clinical Practice in Diabetes ManagementDokument40 SeitenFrom Evidence to Clinical Practice in Diabetes ManagementscribdNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- DMB DNG 2014 Su AdvanceDokument42 SeitenDMB DNG 2014 Su AdvancescribdNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Basic Metabolism Per Ho Mped in 2013Dokument44 SeitenBasic Metabolism Per Ho Mped in 2013scribdNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Data Statistik Ujian Peserta S3Dokument18 SeitenData Statistik Ujian Peserta S3scribdNoch keine Bewertungen
- Basal Bolus InsulinDMT22009Dokument92 SeitenBasal Bolus InsulinDMT22009scribdNoch keine Bewertungen
- Metformin at the Core of T2DM TreatmentDokument37 SeitenMetformin at the Core of T2DM TreatmentscribdNoch keine Bewertungen
- Advisory Board PPT (Dr-2. Ida Ayu Kshanti SPPD, KEMD)Dokument29 SeitenAdvisory Board PPT (Dr-2. Ida Ayu Kshanti SPPD, KEMD)scribdNoch keine Bewertungen
- DTU Slides023AcarboseDokument19 SeitenDTU Slides023AcarbosescribdNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Jafes 28-01-Oa-08 Eb Deliberation FormDokument1 SeiteJafes 28-01-Oa-08 Eb Deliberation FormscribdNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- PDCI Core Kit 15 Indications For Referral of Complex PatientsDokument49 SeitenPDCI Core Kit 15 Indications For Referral of Complex PatientsscribdNoch keine Bewertungen
- Unmet Needs in Diabetes: Present and Future From Clinical PracticeDokument53 SeitenUnmet Needs in Diabetes: Present and Future From Clinical PracticescribdNoch keine Bewertungen
- Obat Rujuk BalikDokument54 SeitenObat Rujuk BalikscribdNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Jafes 28 01 Oa 08 AbstractDokument2 SeitenJafes 28 01 Oa 08 AbstractscribdNoch keine Bewertungen
- Unmet Needs in Diabetes: Present and Future From Clinical PracticeDokument53 SeitenUnmet Needs in Diabetes: Present and Future From Clinical PracticescribdNoch keine Bewertungen
- Makalah Prof Pradana Challenges in Diabetes Management in Indonesia (BioMed 2013)Dokument20 SeitenMakalah Prof Pradana Challenges in Diabetes Management in Indonesia (BioMed 2013)scribdNoch keine Bewertungen
- Dtu Slides022ukpds PTMDokument14 SeitenDtu Slides022ukpds PTMscribdNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Dtu Slides004ukpdsDokument12 SeitenDtu Slides004ukpdsscribdNoch keine Bewertungen
- Does Family History of Obesity, Cardiovascular, and Metabolic Diseases Influence Onset and Severity of Childhood ObesityDokument6 SeitenDoes Family History of Obesity, Cardiovascular, and Metabolic Diseases Influence Onset and Severity of Childhood ObesityTony Miguel Saba SabaNoch keine Bewertungen
- Inositol - Benefits, Side Effects and DosageDokument14 SeitenInositol - Benefits, Side Effects and DosageAri Sa FaNoch keine Bewertungen
- Obesity Diagnosis ManagementDokument26 SeitenObesity Diagnosis ManagementAdán 'Olveera100% (1)
- Chapter 22: Young Adult Edelman: Health Promotion Throughout The Life Span, 8th EditionDokument10 SeitenChapter 22: Young Adult Edelman: Health Promotion Throughout The Life Span, 8th Editionmarvado10100% (1)
- Obesity & Anaesthesia: Co-Ordinator - Dr. Chavi Sethi (MD) Speaker - Dr. Uday Pratap SinghDokument56 SeitenObesity & Anaesthesia: Co-Ordinator - Dr. Chavi Sethi (MD) Speaker - Dr. Uday Pratap SinghRafi ramdhanNoch keine Bewertungen
- Acellular CarbsDokument15 SeitenAcellular CarbsstarmittNoch keine Bewertungen
- DR Sinatra HEART, HEALTH & NUTRITIONDokument8 SeitenDR Sinatra HEART, HEALTH & NUTRITIONalekad65100% (2)
- Correlation Between Hba1c Level and Epicardial Fat Thickness in Acute Coronary Syndrome PatientDokument5 SeitenCorrelation Between Hba1c Level and Epicardial Fat Thickness in Acute Coronary Syndrome PatientIJAR JOURNALNoch keine Bewertungen
- IM Written Report Diabetes Case ReportDokument10 SeitenIM Written Report Diabetes Case ReportJessa Mateum VallangcaNoch keine Bewertungen
- Diabetes MayersDokument14 SeitenDiabetes MayersYisneyNoch keine Bewertungen
- Overview of Medical Care in Adults With Diabetes Mellitus - UpToDate PDFDokument47 SeitenOverview of Medical Care in Adults With Diabetes Mellitus - UpToDate PDFIzamar RomeroNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Andropause: Current Concepts: Keywords: Androgen Deficiency in Ageing Male, Late Onset Hypogonadism, TestosteroneDokument14 SeitenAndropause: Current Concepts: Keywords: Androgen Deficiency in Ageing Male, Late Onset Hypogonadism, TestosteroneYariCárdenasNoch keine Bewertungen
- Jurnal Stroke 2017 PDFDokument25 SeitenJurnal Stroke 2017 PDFSinta AgustinaNoch keine Bewertungen
- The 8 Second Secret The Scientifically Proven Method For Lasting WeightlossDokument204 SeitenThe 8 Second Secret The Scientifically Proven Method For Lasting WeightlossGlen HutchinsonNoch keine Bewertungen
- Molecular Mechanisms of Adipogenesis in Obesity and The Metabolic SyndromeDokument144 SeitenMolecular Mechanisms of Adipogenesis in Obesity and The Metabolic SyndromesserggiosNoch keine Bewertungen
- Cardiometabolic Syndrome: & DR Dhafir A. MahmoodDokument62 SeitenCardiometabolic Syndrome: & DR Dhafir A. MahmoodJacob AlphaNoch keine Bewertungen
- Stephen Holt MD-Integrative Medicine Definitions and InitiativesDokument23 SeitenStephen Holt MD-Integrative Medicine Definitions and InitiativesStephen Holt MD100% (3)
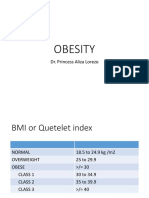
- Obesity: Dr. Princess Aliza LorezoDokument13 SeitenObesity: Dr. Princess Aliza LorezorosamundraeNoch keine Bewertungen
- Fact Sheeton Canola OilDokument15 SeitenFact Sheeton Canola OilMonika ThadeaNoch keine Bewertungen
- The Paleo Manifesto by John Durant - ExcerptDokument17 SeitenThe Paleo Manifesto by John Durant - ExcerptCrown Publishing GroupNoch keine Bewertungen
- Effect of Calorie Restriction and Exercise On Type 2 DiabetesDokument18 SeitenEffect of Calorie Restriction and Exercise On Type 2 DiabetesDitya Monica 065Noch keine Bewertungen
- Diabtec Book enDokument192 SeitenDiabtec Book enÐя.Randa AbozaidNoch keine Bewertungen
- NTRN 516 Case Study 2 - DM 10 12 15 UpdateDokument18 SeitenNTRN 516 Case Study 2 - DM 10 12 15 Updateapi-315324296Noch keine Bewertungen
- Rising Incidence of Overweight and Obesity Among Children and Adolescents in IndiaDokument8 SeitenRising Incidence of Overweight and Obesity Among Children and Adolescents in IndiaSSR-IIJLS JournalNoch keine Bewertungen
- Diabetes Mellitus LECTURE Yr IIIDokument27 SeitenDiabetes Mellitus LECTURE Yr IIIMwanja Moses100% (1)
- Chapter 13 Quiz For Health Psychology 328 McgillDokument3 SeitenChapter 13 Quiz For Health Psychology 328 McgillOlivia CoutoNoch keine Bewertungen
- 040-444 ACSM Registered Clinical Exercise PhysiologistDokument101 Seiten040-444 ACSM Registered Clinical Exercise PhysiologistKamran MusaNoch keine Bewertungen
- Pathophysiology and Pathogenesis of Type 2 DiabetesDokument8 SeitenPathophysiology and Pathogenesis of Type 2 DiabetesGladys SorianoNoch keine Bewertungen
- Anti Inflammatory Diets 2015Dokument9 SeitenAnti Inflammatory Diets 2015twice againNoch keine Bewertungen
- Pcos Ob JournalDokument10 SeitenPcos Ob JournalSean SialanaNoch keine Bewertungen