Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- MemantineDokument7 SeitenMemantineroboNoch keine Bewertungen
- GEHC Site Planning Specifications Safety and Specifications PDFDokument57 SeitenGEHC Site Planning Specifications Safety and Specifications PDFD&KNoch keine Bewertungen
- Philosophy of OcclusionDokument23 SeitenPhilosophy of OcclusionAnil SukumaranNoch keine Bewertungen
- 5th Handbook of Transfusion MedicineDokument186 Seiten5th Handbook of Transfusion MedicineDokter Dhea Danni Agisty100% (1)
- Unmet Needs in Diabetes: Present and Future From Clinical PracticeDokument53 SeitenUnmet Needs in Diabetes: Present and Future From Clinical PracticescribdNoch keine Bewertungen
- Unmet Needs in Diabetes: Present and Future From Clinical PracticeDokument53 SeitenUnmet Needs in Diabetes: Present and Future From Clinical PracticescribdNoch keine Bewertungen
- Trees in IndiaDokument43 SeitenTrees in IndiaAr Archana PrabakaranNoch keine Bewertungen
- PERIMETRY Introduction GuideDokument70 SeitenPERIMETRY Introduction GuideDana Andreea Popescu100% (1)
- Cholelithiasis SampleDokument77 SeitenCholelithiasis Samplekrischamcute67% (3)
- Basal Bolus InsulinDMT22009Dokument92 SeitenBasal Bolus InsulinDMT22009scribdNoch keine Bewertungen
- Torque in Orthodontics A Review March 2022 7544320615 0608221Dokument3 SeitenTorque in Orthodontics A Review March 2022 7544320615 0608221chaitreeNoch keine Bewertungen
- 10 Hip Replacement SurgeryDokument13 Seiten10 Hip Replacement SurgeryDIA PHONG THANGNoch keine Bewertungen
- Diana Sanchez V City & County of DenverDokument48 SeitenDiana Sanchez V City & County of DenverEllyn SantiagoNoch keine Bewertungen
- Shangri-La JKT - JDMDokument2 SeitenShangri-La JKT - JDMscribdNoch keine Bewertungen
- Unmet Need DM Management in Primary Care Seting 280914Dokument62 SeitenUnmet Need DM Management in Primary Care Seting 280914scribdNoch keine Bewertungen
- Ways To Improve The Macrovascular Outcomes in Type 2 Diabetes TherapyDokument42 SeitenWays To Improve The Macrovascular Outcomes in Type 2 Diabetes TherapyscribdNoch keine Bewertungen
- PDCI Core Kit 15 Indications For Referral of Complex PatientsDokument49 SeitenPDCI Core Kit 15 Indications For Referral of Complex PatientsscribdNoch keine Bewertungen
- Diabetes Care in Indonesia - Role of GLP 1 Analog: Pradana SoewondoDokument58 SeitenDiabetes Care in Indonesia - Role of GLP 1 Analog: Pradana SoewondoscribdNoch keine Bewertungen
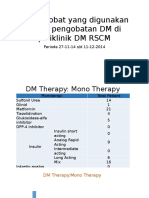
- Survey Obat DM Poli Endokrin (Prof - Sarwono)Dokument8 SeitenSurvey Obat DM Poli Endokrin (Prof - Sarwono)scribdNoch keine Bewertungen
- Sist - Penelitian ProDokument57 SeitenSist - Penelitian ProscribdNoch keine Bewertungen
- Current Concepts of Chronic Diabetic ComplicationsDokument4 SeitenCurrent Concepts of Chronic Diabetic ComplicationsscribdNoch keine Bewertungen
- DMB DNG 2014 Su AdvanceDokument42 SeitenDMB DNG 2014 Su AdvancescribdNoch keine Bewertungen
- Workshop: Case StudyDokument28 SeitenWorkshop: Case StudyscribdNoch keine Bewertungen
- DMcombos JDM2014Dokument5 SeitenDMcombos JDM2014scribdNoch keine Bewertungen
- DMCombos JDM2014Dokument160 SeitenDMCombos JDM2014scribdNoch keine Bewertungen
- Management of Type 2 Diabetes: Should Metformin Be at The Core of Treatment Guidelines?Dokument37 SeitenManagement of Type 2 Diabetes: Should Metformin Be at The Core of Treatment Guidelines?scribdNoch keine Bewertungen
- From Evidence Based To Clinical Practice in Type 2 Diabetes MellitusDokument40 SeitenFrom Evidence Based To Clinical Practice in Type 2 Diabetes MellitusscribdNoch keine Bewertungen
- Advisory Board PPT (Dr-2. Ida Ayu Kshanti SPPD, KEMD)Dokument29 SeitenAdvisory Board PPT (Dr-2. Ida Ayu Kshanti SPPD, KEMD)scribdNoch keine Bewertungen
- PDCI Core Kit 15 Indications For Referral of Complex PatientsDokument49 SeitenPDCI Core Kit 15 Indications For Referral of Complex PatientsscribdNoch keine Bewertungen
- Data Statistik Ujian Peserta S3Dokument18 SeitenData Statistik Ujian Peserta S3scribdNoch keine Bewertungen
- Basic Metabolism Per Ho Mped in 2013Dokument44 SeitenBasic Metabolism Per Ho Mped in 2013scribdNoch keine Bewertungen
- DTU Slides023AcarboseDokument19 SeitenDTU Slides023AcarbosescribdNoch keine Bewertungen
- Jafes 28-01-Oa-08 Eb Deliberation FormDokument1 SeiteJafes 28-01-Oa-08 Eb Deliberation FormscribdNoch keine Bewertungen
- Obat Rujuk BalikDokument54 SeitenObat Rujuk BalikscribdNoch keine Bewertungen
- Makalah Prof Pradana Challenges in Diabetes Management in Indonesia (BioMed 2013)Dokument20 SeitenMakalah Prof Pradana Challenges in Diabetes Management in Indonesia (BioMed 2013)scribdNoch keine Bewertungen
- Dtu Slides004ukpdsDokument12 SeitenDtu Slides004ukpdsscribdNoch keine Bewertungen
- Jafes 28 01 Oa 08 AbstractDokument2 SeitenJafes 28 01 Oa 08 AbstractscribdNoch keine Bewertungen
- Dtu Slides022ukpds PTMDokument14 SeitenDtu Slides022ukpds PTMscribdNoch keine Bewertungen
- Metabolic Problems and Vascular Disease: Sarwono WaspadjiDokument58 SeitenMetabolic Problems and Vascular Disease: Sarwono WaspadjiscribdNoch keine Bewertungen
- Item Balance Per Unit RPTDokument60 SeitenItem Balance Per Unit RPTYogie 1290Noch keine Bewertungen
- Tenets and Codes of ConductDokument128 SeitenTenets and Codes of ConductRodolf Dominic Serafin R. RobledoNoch keine Bewertungen
- Scientific Agenda 1st PAEC Virtual Breast Cancer Symposium 15-10-2022Dokument4 SeitenScientific Agenda 1st PAEC Virtual Breast Cancer Symposium 15-10-2022M NaveedNoch keine Bewertungen
- ADR Form PDFDokument2 SeitenADR Form PDFCha Tuban DianaNoch keine Bewertungen
- Crisis HiperglicémicaDokument31 SeitenCrisis HiperglicémicaMelany Esteban BarzolaNoch keine Bewertungen
- Reasons For Extraction of Primary Teeth in Jordan-A Study.: August 2013Dokument5 SeitenReasons For Extraction of Primary Teeth in Jordan-A Study.: August 2013Mutia KumalasariNoch keine Bewertungen
- International Journal of PharmaceuticsDokument6 SeitenInternational Journal of PharmaceuticsSjis11362Noch keine Bewertungen
- Parkinsons Presentation Case StudyDokument33 SeitenParkinsons Presentation Case Studyapi-287759747Noch keine Bewertungen
- Typhoid Fever at A GlanceDokument2 SeitenTyphoid Fever at A GlanceLIZNoch keine Bewertungen
- EDIC Guidelines 2017 PDFDokument22 SeitenEDIC Guidelines 2017 PDFZia ShaikhNoch keine Bewertungen
- Reliance Policy Extn Request FormDokument1 SeiteReliance Policy Extn Request Formanshu_204Noch keine Bewertungen
- Medication Card CelebrexDokument2 SeitenMedication Card CelebrexTSPAN100% (1)
- Full Text of PT-OT Exam Results (Top 10)Dokument2 SeitenFull Text of PT-OT Exam Results (Top 10)TheSummitExpressNoch keine Bewertungen
- Tetracycline, Doxycycline, minocycline-Tetracyclines-InfenctionsDokument1 SeiteTetracycline, Doxycycline, minocycline-Tetracyclines-InfenctionsNatalia SpencerNoch keine Bewertungen
- Pharmacy Practice Sample ReportDokument26 SeitenPharmacy Practice Sample Reportsaransh misraNoch keine Bewertungen
- Classification of Drugs Are: Hepatoprotective Drugs E.g.: Silymarin Antibiotics E.G.Dokument2 SeitenClassification of Drugs Are: Hepatoprotective Drugs E.g.: Silymarin Antibiotics E.G.Navya Sara SanthoshNoch keine Bewertungen
- Curriculum Vitae: Dr. Avinash K. Jangde - . - ., - . (A)Dokument5 SeitenCurriculum Vitae: Dr. Avinash K. Jangde - . - ., - . (A)Mohammad TariqNoch keine Bewertungen
- Procalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsDokument2 SeitenProcalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsMr. LNoch keine Bewertungen
- Langerhans-Cell Histiocytosis: Review ArticleDokument13 SeitenLangerhans-Cell Histiocytosis: Review ArticleHanifah ArroziNoch keine Bewertungen
- Media Contact: Lexie Murray, PR Manager - 512. 609. 8017 X 105Dokument3 SeitenMedia Contact: Lexie Murray, PR Manager - 512. 609. 8017 X 105sNoch keine Bewertungen