Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- UROLOGYDokument222 SeitenUROLOGYBeso DavitashviliNoch keine Bewertungen
- Stones, Urinary Stones or Renal Calculi. As Aforementioned, It Is Quite Vague andDokument4 SeitenStones, Urinary Stones or Renal Calculi. As Aforementioned, It Is Quite Vague andChristian Salunga SangalangNoch keine Bewertungen
- Acute Kidney InjuryDokument35 SeitenAcute Kidney InjuryMuhrawi Yunding100% (1)
- Urinay SystemDokument14 SeitenUrinay SystemAficionadoNoch keine Bewertungen
- Test Bank For Medical Terminology A Living Language 7th Edition by Fremgen Full DownloadDokument47 SeitenTest Bank For Medical Terminology A Living Language 7th Edition by Fremgen Full Downloadjamesacostaowjrfctxdk100% (16)
- Biology Form 5 - The Human Urinary SystemDokument50 SeitenBiology Form 5 - The Human Urinary Systemilykhairunnisa0% (1)
- Banerji Protocol 6Dokument4 SeitenBanerji Protocol 6Sandip ChatterjeeNoch keine Bewertungen
- Manna-UTI Quizlet DSDokument3 SeitenManna-UTI Quizlet DSBlessing KelechiNoch keine Bewertungen
- Reproductive SystemDokument7 SeitenReproductive Systemcollege code - 5Noch keine Bewertungen
- 1st Long Quiz in Science 5Dokument27 Seiten1st Long Quiz in Science 5ARIEL JAY CHICONoch keine Bewertungen
- Histology Male ReproductiveDokument31 SeitenHistology Male Reproductivekhiks34Noch keine Bewertungen
- La Salle University Nursing Care PlanDokument3 SeitenLa Salle University Nursing Care PlanJb RosillosaNoch keine Bewertungen
- Histology of Male Reproductive SystemDokument56 SeitenHistology of Male Reproductive SystemMuhammad Irfan100% (2)
- ADH Diagram AnimatedDokument8 SeitenADH Diagram AnimatedCarl Agape DavisNoch keine Bewertungen
- UtiDokument2 SeitenUtiBasant karn50% (2)
- 4.physiology of Micturition PDFDokument20 Seiten4.physiology of Micturition PDFNaimish VermaNoch keine Bewertungen
- Ncma217 Lec PrelimDokument38 SeitenNcma217 Lec PrelimIVY SUPNETNoch keine Bewertungen
- Batu Ren, Batu Ureter Dan Onko NewDokument29 SeitenBatu Ren, Batu Ureter Dan Onko Newilham masdarNoch keine Bewertungen
- Chapter 24 Urinary BladderDokument42 SeitenChapter 24 Urinary BladderMACON824Noch keine Bewertungen
- RRM's Next - Urology-Penis & UrethraDokument32 SeitenRRM's Next - Urology-Penis & UrethrairfanNoch keine Bewertungen
- Male Reproductive SystemDokument32 SeitenMale Reproductive SystemManilyn PenafloridaNoch keine Bewertungen
- 40 TS1M1 Sex and Sexuality-Vol. 2 (Praeger 2006)Dokument289 Seiten40 TS1M1 Sex and Sexuality-Vol. 2 (Praeger 2006)bfdscaNoch keine Bewertungen
- Check List of Urinary Catheterization For EMT LevelDokument12 SeitenCheck List of Urinary Catheterization For EMT LevelFikir Ligisinaw AyalkimNoch keine Bewertungen
- Visual Internal Urethrotomy For Adult Male UrethraDokument6 SeitenVisual Internal Urethrotomy For Adult Male UrethraGd SuarantaNoch keine Bewertungen
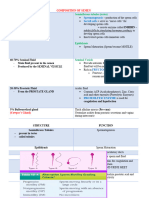
- Composition of SemenDokument15 SeitenComposition of SemenSamantha IsabelNoch keine Bewertungen
- The Male Reproductive SystemDokument5 SeitenThe Male Reproductive SystemTamie P. GalindoNoch keine Bewertungen
- Testicular Examination OSCE GuideDokument9 SeitenTesticular Examination OSCE Guidecharlyn206Noch keine Bewertungen
- Male GU ExamDokument5 SeitenMale GU ExamOmar Farid ElgebalyNoch keine Bewertungen
- Anatomy and Physiology: Patient P / Room No. 415 - 1Dokument3 SeitenAnatomy and Physiology: Patient P / Room No. 415 - 1Julianne B. Dela Cruz100% (1)
- Nursing Care PlanDokument1 SeiteNursing Care PlanSHeenah Qo100% (1)