Das könnte Ihnen auch gefallen
- Gram Positive BacilliDokument9 SeitenGram Positive BacilliRovy JervisNoch keine Bewertungen
- Sir Alvin Rey Flores: Echinococcus Granulosus, Taenia Solium)Dokument5 SeitenSir Alvin Rey Flores: Echinococcus Granulosus, Taenia Solium)Corin LimNoch keine Bewertungen
- CLINICAL CHEMISTRY: Passbooks Study GuideVon EverandCLINICAL CHEMISTRY: Passbooks Study GuideNoch keine Bewertungen
- Staphylococcus LectureDokument66 SeitenStaphylococcus LectureFarhan Azmain FahimNoch keine Bewertungen
- Staphylococcus Spp. Gram Positive. ClusteredDokument15 SeitenStaphylococcus Spp. Gram Positive. ClusteredIvy NNoch keine Bewertungen
- Bacte TestDokument10 SeitenBacte TestRiondalionNoch keine Bewertungen
- Medical Parasitology - FullDokument30 SeitenMedical Parasitology - FullJesse Osborn100% (2)
- Coagulation NotesDokument14 SeitenCoagulation NotesthrowawyNoch keine Bewertungen
- Intro To Mycology Prelims2Dokument47 SeitenIntro To Mycology Prelims2Annika AbadNoch keine Bewertungen
- Test Request Form - (Name Laboratory) : Patient Details Requester DetailsDokument1 SeiteTest Request Form - (Name Laboratory) : Patient Details Requester DetailsMisty Collings100% (1)
- The Medically Important MycosesDokument8 SeitenThe Medically Important MycosesNatasha JeanNoch keine Bewertungen
- Preoperative Management of Patients Undergoing AnaesthesiaDokument24 SeitenPreoperative Management of Patients Undergoing AnaesthesiaGx NavinNoch keine Bewertungen
- ENTEROBACTERIACEAE2Dokument14 SeitenENTEROBACTERIACEAE2dokijoon100% (1)
- Microbiology Memorization SheetDokument5 SeitenMicrobiology Memorization Sheetalobrien100% (1)
- Summary of Diagnostic BacteriologyDokument45 SeitenSummary of Diagnostic Bacteriologyomaromran100% (3)
- StreptococcusDokument6 SeitenStreptococcusAyessa VillacorteNoch keine Bewertungen
- Microbiology ChartsDokument17 SeitenMicrobiology Chartsclower112Noch keine Bewertungen
- Modul Perfect Score SBP Chemistry SPM 2013Dokument151 SeitenModul Perfect Score SBP Chemistry SPM 2013Cikgu Faizal100% (15)
- Microb Summary 3314Dokument28 SeitenMicrob Summary 3314KPNoch keine Bewertungen
- MycoViro 2Dokument44 SeitenMycoViro 2Ria AlcantaraNoch keine Bewertungen
- Microbiology 200 PointsDokument11 SeitenMicrobiology 200 PointsHassan AhmadNoch keine Bewertungen
- A. Staphylococcus Aureus B. Staphylococcus Epidermidis C. Staphylococcus SaprophyticusDokument8 SeitenA. Staphylococcus Aureus B. Staphylococcus Epidermidis C. Staphylococcus SaprophyticusRuel MaddawinNoch keine Bewertungen
- BacteriaDokument13 SeitenBacteriathzone1986Noch keine Bewertungen
- Mycology Shereena V. Opiniano, RMT, MSMT. Terms: Saprobes Symbionts Asexual Types: A. SporangiosporesDokument7 SeitenMycology Shereena V. Opiniano, RMT, MSMT. Terms: Saprobes Symbionts Asexual Types: A. SporangiosporesStephie Mae100% (1)
- Clinical Bacteriology ReviewerDokument17 SeitenClinical Bacteriology Reviewer99noname100% (1)
- CompilationDokument3 SeitenCompilationBelle Cherlette FelipeNoch keine Bewertungen
- Herpes, Pox, Rhabdo, Arena VIRUSDokument7 SeitenHerpes, Pox, Rhabdo, Arena VIRUSErnie G. Bautista II, RN, MDNoch keine Bewertungen
- Ricketsiae BacteriaDokument2 SeitenRicketsiae BacteriaErnie G. Bautista II, RN, MDNoch keine Bewertungen
- Plant Anatomy and PhysiologyDokument33 SeitenPlant Anatomy and Physiologymneilg100% (1)
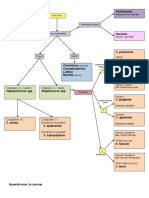
- Flow Chart of Gram Negative OrganismsDokument1 SeiteFlow Chart of Gram Negative OrganismsKristine Marie PateñoNoch keine Bewertungen
- Gram Positive Cocci Sem 1 1Dokument45 SeitenGram Positive Cocci Sem 1 1Charmaine Corpuz Granil100% (1)
- Bacteriology SummaryDokument35 SeitenBacteriology SummarykevinNoch keine Bewertungen
- Microbiology Revision E6.5Dokument132 SeitenMicrobiology Revision E6.5massprithiv58Noch keine Bewertungen
- Microbiology, Bailey - S and Scotts Chapter 28, Moraxella and Related Orgs. by MT1232Dokument3 SeitenMicrobiology, Bailey - S and Scotts Chapter 28, Moraxella and Related Orgs. by MT1232Aisle Malibiran PalerNoch keine Bewertungen
- Microbiology: Presented by Alyazeed Hussein, BSCDokument64 SeitenMicrobiology: Presented by Alyazeed Hussein, BSCT N100% (1)
- Parraetal ForensicScienceandHumanitarianAction 2020Dokument847 SeitenParraetal ForensicScienceandHumanitarianAction 2020Sofia ChacaltanaNoch keine Bewertungen
- Gram Negative RodsDokument8 SeitenGram Negative RodsRuel Maddawin100% (1)
- Mycobacteria: Nocardia, Rhodococcus, Tsukamurella and GordoniaDokument7 SeitenMycobacteria: Nocardia, Rhodococcus, Tsukamurella and Gordonia20C – Gorospe, Rhai Chezka V.Noch keine Bewertungen
- Clinical Neurovirology PDFDokument661 SeitenClinical Neurovirology PDFpitumestresNoch keine Bewertungen
- Bacte Day 2Dokument24 SeitenBacte Day 2Jadey InfanteNoch keine Bewertungen
- Aubf Lab CSFDokument6 SeitenAubf Lab CSFAndrei Tumarong AngoluanNoch keine Bewertungen
- (Microbio) Staphyloccocus and Streptococcus-Dr. Salandanan (BHND)Dokument16 Seiten(Microbio) Staphyloccocus and Streptococcus-Dr. Salandanan (BHND)Lee Delos Santos100% (1)
- Mega Micro para Table 1 (1) (PDF - Io)Dokument81 SeitenMega Micro para Table 1 (1) (PDF - Io)CheryldaneBaculiNoch keine Bewertungen
- Practical 4 Staphylococci PresentationDokument24 SeitenPractical 4 Staphylococci PresentationPatrisha BuanNoch keine Bewertungen
- Me EnterobacteriaceaeDokument72 SeitenMe Enterobacteriaceaewimarshana gamage100% (1)
- Review Parasitology ChartsDokument8 SeitenReview Parasitology Chartseezah100% (2)
- Bacteria Associated With GIT Infections I TableDokument4 SeitenBacteria Associated With GIT Infections I Tablekris0% (1)
- Ent Emergencies NKDokument39 SeitenEnt Emergencies NKGx NavinNoch keine Bewertungen
- Cytopathologic Diagnosis of Serous Fluids - Shidham & AtkinsonDokument9 SeitenCytopathologic Diagnosis of Serous Fluids - Shidham & Atkinsonvshidham100% (1)
- Staphylococci: Streptococcus PyogenesDokument20 SeitenStaphylococci: Streptococcus PyogenesPharmacy2015100% (2)
- Major Bacterial Genera Table For ReviewDokument12 SeitenMajor Bacterial Genera Table For ReviewmojdaNoch keine Bewertungen
- Serological TestsDokument2 SeitenSerological TestsKimberly EspaldonNoch keine Bewertungen
- Microbiology - ParasitologyDokument34 SeitenMicrobiology - ParasitologySasi DharanNoch keine Bewertungen
- Anaerobe of Clinical ImportanceDokument43 SeitenAnaerobe of Clinical ImportanceDayledaniel SorvetoNoch keine Bewertungen
- (Bacteriology) Chapter 8: Use of Colonial Morphology For The Presumptive Identification of MicroorganismsDokument6 Seiten(Bacteriology) Chapter 8: Use of Colonial Morphology For The Presumptive Identification of MicroorganismsJean BelciñaNoch keine Bewertungen
- Biochemical TestsDokument2 SeitenBiochemical TestsVishnu Reddy Vardhan PulimiNoch keine Bewertungen
- Microbiology CaseDokument3 SeitenMicrobiology Caseclower112100% (2)
- Bacteriology SummaryDokument38 SeitenBacteriology SummaryMohsen HaleemNoch keine Bewertungen
- Clinical Microscopy: Definition and Volume Disease and Cause PolyuriaDokument5 SeitenClinical Microscopy: Definition and Volume Disease and Cause PolyuriaJovanni andesNoch keine Bewertungen
- Microbiology List of BacteriaDokument5 SeitenMicrobiology List of BacteriaJaweria Islam Khan BangashNoch keine Bewertungen
- SubcutaneousDokument2 SeitenSubcutaneousMary ChristelleNoch keine Bewertungen
- Chapter 2 Introduction To Urinalysis PDFDokument4 SeitenChapter 2 Introduction To Urinalysis PDFJulie Anne Soro ValdezNoch keine Bewertungen
- Summary of Reagent Strip TestsDokument8 SeitenSummary of Reagent Strip TestsDarla YsavelNoch keine Bewertungen
- AnemiaDokument9 SeitenAnemiaMila Canoza HerreraNoch keine Bewertungen
- MicrobiologyDokument49 SeitenMicrobiologyinnyNoch keine Bewertungen
- MedtechDokument7 SeitenMedtechLyudmyla GillegoNoch keine Bewertungen
- Multiple Choice Question (True-False)Dokument10 SeitenMultiple Choice Question (True-False)Gx NavinNoch keine Bewertungen
- Perioperative Care: Nur Azimah Izyan IrdinaDokument42 SeitenPerioperative Care: Nur Azimah Izyan IrdinaGx Navin100% (2)
- Special Forms of PeritonitisDokument10 SeitenSpecial Forms of PeritonitisGx NavinNoch keine Bewertungen
- Abd Wall - Inguinal Reg. - Upnm7 - 210218Dokument38 SeitenAbd Wall - Inguinal Reg. - Upnm7 - 210218Gx NavinNoch keine Bewertungen
- Systemic Approach in Intensive Care MedicineDokument16 SeitenSystemic Approach in Intensive Care MedicineGx NavinNoch keine Bewertungen
- Iud PPT ColorDokument47 SeitenIud PPT ColorYonaziraNoch keine Bewertungen
- Json Software LicenseDokument1 SeiteJson Software LicenseGx NavinNoch keine Bewertungen
- Activity 3Dokument5 SeitenActivity 3Gx NavinNoch keine Bewertungen
- Sgs 11 - TB & Asthma4Dokument13 SeitenSgs 11 - TB & Asthma4Gx NavinNoch keine Bewertungen
- Genetics in HematologyDokument33 SeitenGenetics in HematologyGx NavinNoch keine Bewertungen
- KPP Book EngDokument160 SeitenKPP Book EngSora Mayonaka100% (1)
- Inguinal Region 1617Dokument23 SeitenInguinal Region 1617Gx NavinNoch keine Bewertungen
- MSDS SD 118Dokument8 SeitenMSDS SD 118Gx Navin0% (1)
- Json Software LicenseDokument1 SeiteJson Software LicenseGx NavinNoch keine Bewertungen
- LicenseDokument6 SeitenLicensemerrysun22Noch keine Bewertungen
- SUTHESANDokument10 SeitenSUTHESANGx NavinNoch keine Bewertungen
- Another Study Showing An Increased Risk For Cancer With Drinking AlcoholDokument2 SeitenAnother Study Showing An Increased Risk For Cancer With Drinking AlcoholGx NavinNoch keine Bewertungen
- Presentation 9Dokument2 SeitenPresentation 9Gx NavinNoch keine Bewertungen
- Flight Booking NumberDokument1 SeiteFlight Booking NumberGx NavinNoch keine Bewertungen
- LicenseDokument6 SeitenLicensemerrysun22Noch keine Bewertungen
- 5 Words Per DayDokument1 Seite5 Words Per DayGx NavinNoch keine Bewertungen
- 5 Words Per DayDokument1 Seite5 Words Per DayGx NavinNoch keine Bewertungen
- PMR Percubaan 2009 Pahang English LanguageDokument17 SeitenPMR Percubaan 2009 Pahang English LanguageChinWynn.com100% (1)
- Caring For The ElderyDokument1 SeiteCaring For The ElderyGx NavinNoch keine Bewertungen
- Answering Techniques For SPM 2010 Biology Paper 3Dokument11 SeitenAnswering Techniques For SPM 2010 Biology Paper 3Ong Chee KiongNoch keine Bewertungen
- Bahasa Inggeris P1 Trial PMR Perak 2009Dokument12 SeitenBahasa Inggeris P1 Trial PMR Perak 2009HaFez Hisham100% (3)
- The Assessment of Post-Vasecto PDFDokument10 SeitenThe Assessment of Post-Vasecto PDFapek leeNoch keine Bewertungen
- Biochemistry CO PoisoningDokument19 SeitenBiochemistry CO PoisoningHann SantiagoNoch keine Bewertungen
- LP OkDokument10 SeitenLP OkHannah Rose ValdezNoch keine Bewertungen
- Ain Aging and Neurodegeneration 1998 EbookDokument267 SeitenAin Aging and Neurodegeneration 1998 EbookbebleffNoch keine Bewertungen
- Dengue PPT YaarDokument21 SeitenDengue PPT YaarY ShouryaNoch keine Bewertungen
- Guna Draft Study Full ReportDokument64 SeitenGuna Draft Study Full ReportAbeje Zewdie88% (8)
- Activity 3 - The Human ReflexDokument2 SeitenActivity 3 - The Human ReflexGOOKIEBOONoch keine Bewertungen
- Principles of Microbial Alchemy - Insights From The Streptomyces Coelicolor Genome Sequence PDFDokument5 SeitenPrinciples of Microbial Alchemy - Insights From The Streptomyces Coelicolor Genome Sequence PDFCaesar VranceanuNoch keine Bewertungen
- Lab Report IDokument11 SeitenLab Report IElle B.Noch keine Bewertungen
- ESCMC Catalogo Da BibliotecaDokument141 SeitenESCMC Catalogo Da Bibliotecaeusoqueroessapesquis0% (1)
- ItemDokument254 SeitenItemdlc352-sc1Noch keine Bewertungen
- 19 - 2010 Elevação Do Nível de Consciência em Guandu - Uma Perspectiva GlobalDokument542 Seiten19 - 2010 Elevação Do Nível de Consciência em Guandu - Uma Perspectiva GlobaldenissatoNoch keine Bewertungen
- Coordination CPPDokument8 SeitenCoordination CPPSri KrishnaNoch keine Bewertungen
- 4a Lesson PlanDokument10 Seiten4a Lesson PlanPauline E. BinarabaNoch keine Bewertungen
- Activity - Camera and Human EyeDokument5 SeitenActivity - Camera and Human EyeVincee SamsonNoch keine Bewertungen
- Biotechnology Reports: Alireza Zakeri, Mohammad Javad Rasaee, Navid PourzardoshtDokument6 SeitenBiotechnology Reports: Alireza Zakeri, Mohammad Javad Rasaee, Navid PourzardoshtNancyHendryNoch keine Bewertungen
- Jurnal: PERBANYAKAN AKASIA HIBRIDA (Acacia Mangium × AcaciaDokument14 SeitenJurnal: PERBANYAKAN AKASIA HIBRIDA (Acacia Mangium × AcaciaTT ZmDESNoch keine Bewertungen
- Edible Plants: Eduardo H. Rapoport and Barbara S. DrausalDokument8 SeitenEdible Plants: Eduardo H. Rapoport and Barbara S. DrausalrafrejuNoch keine Bewertungen
- 14 - Interferences in Immunoassay PDFDokument16 Seiten14 - Interferences in Immunoassay PDFLyannYisellNoch keine Bewertungen
- Isopod BehaviorDokument4 SeitenIsopod BehaviorCody Griffin100% (1)
- Laboratory Manual For Anatomy and Physiology 6th Edition Marieb Solutions ManualDokument26 SeitenLaboratory Manual For Anatomy and Physiology 6th Edition Marieb Solutions ManualAlexMartinxfgr100% (56)
- 9 y GLDokument3 Seiten9 y GLAgz ThefnanNoch keine Bewertungen
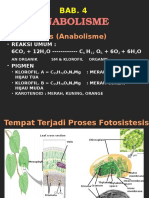
- Bab.4. AnabolismeDokument14 SeitenBab.4. AnabolismeSurniSajaNoch keine Bewertungen
- Physical Education Class 11 Short Answers Chapter 8Dokument3 SeitenPhysical Education Class 11 Short Answers Chapter 8Peyush NeneNoch keine Bewertungen
- Adult Development and Aging Biopsychosocial Perspectives Canadian 1st Edition Whitbourne Test BankDokument18 SeitenAdult Development and Aging Biopsychosocial Perspectives Canadian 1st Edition Whitbourne Test BankAlanHolmesgnbdp100% (15)