Das könnte Ihnen auch gefallen
- Indirect OphthalmosDokument44 SeitenIndirect Ophthalmosshar_s85Noch keine Bewertungen
- Optigal's Q & A for the NOCE: National Opticianry Certification Exam Questions - Basic CertificationVon EverandOptigal's Q & A for the NOCE: National Opticianry Certification Exam Questions - Basic CertificationNoch keine Bewertungen
- Drugs and the Eye: Sponsored by the British Optical AssociationVon EverandDrugs and the Eye: Sponsored by the British Optical AssociationNoch keine Bewertungen
- The Actions and Uses of Ophthalmic Drugs: A Textbook for Students and PractitionersVon EverandThe Actions and Uses of Ophthalmic Drugs: A Textbook for Students and PractitionersNoch keine Bewertungen
- Visual Field InterpretationDokument52 SeitenVisual Field InterpretationUlquiorra Schiffer100% (1)
- Contact Lens Design Tables: Tables for the Determination of Surface Radii of Curvature of Hard Contact Lenses to Give a Required Axial Edge LiftVon EverandContact Lens Design Tables: Tables for the Determination of Surface Radii of Curvature of Hard Contact Lenses to Give a Required Axial Edge LiftNoch keine Bewertungen
- Dr. Mamta Dept of Ophthalmology RNT Medical College, UdaipurDokument56 SeitenDr. Mamta Dept of Ophthalmology RNT Medical College, UdaipurGideon IrwandaNoch keine Bewertungen
- Contact Applanation TonometryDokument6 SeitenContact Applanation TonometryAmirhosseinSamadzadehNoch keine Bewertungen
- Shyam 2 - ExophthalomometryDokument43 SeitenShyam 2 - Exophthalomometrykshitij Shivhare100% (1)
- Scientific Foundations of OphthalmologyVon EverandScientific Foundations of OphthalmologyEdward S. PerkinsNoch keine Bewertungen
- Ocular Examination and Imaging TechniqueDokument33 SeitenOcular Examination and Imaging TechniqueluckyNoch keine Bewertungen
- Glaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913Von EverandGlaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913Noch keine Bewertungen
- Clinical Study On Scleral Lenses by Dr. Elise KramerDokument8 SeitenClinical Study On Scleral Lenses by Dr. Elise KramerMiami Contact Lens InstituteNoch keine Bewertungen
- Contact Lens GuideDokument45 SeitenContact Lens GuideLigia BoazuNoch keine Bewertungen
- Optical Coherence TomographyDokument82 SeitenOptical Coherence TomographyPutri kartiniNoch keine Bewertungen
- The Retina A Model for Cell Biology Studies Part_1Von EverandThe Retina A Model for Cell Biology Studies Part_1Ruben AdlerNoch keine Bewertungen
- Hey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsVon EverandHey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsNoch keine Bewertungen
- Management of Juvenile Glaucoma With TrabeculectomyDokument147 SeitenManagement of Juvenile Glaucoma With TrabeculectomyErlinaerlin100% (1)
- Basics of FundusDokument29 SeitenBasics of Fundusikayapmd100% (1)
- Retinal Diseases 230210 210855Dokument108 SeitenRetinal Diseases 230210 210855RgdNoch keine Bewertungen
- Cirrus How To Read en OUS en 31 011 0002II Final3Dokument28 SeitenCirrus How To Read en OUS en 31 011 0002II Final3Alondra Verdugo GómezNoch keine Bewertungen
- Cell Biology of the EyeVon EverandCell Biology of the EyeDavid McdevittNoch keine Bewertungen
- Simplifying Strabismus: A Practical Approach to Diagnosis and ManagementVon EverandSimplifying Strabismus: A Practical Approach to Diagnosis and ManagementNoch keine Bewertungen
- Clinical Orthoptics - Fiona Rowe - 146Dokument6 SeitenClinical Orthoptics - Fiona Rowe - 146Danielle SangalangNoch keine Bewertungen
- Optometry Guidelines For Use of Scheduled MedicinesDokument11 SeitenOptometry Guidelines For Use of Scheduled MedicinesJLoNoch keine Bewertungen
- StrabismusDokument32 SeitenStrabismusparugandooNoch keine Bewertungen
- Continue: Stallard's Eye Surgery PDFDokument3 SeitenContinue: Stallard's Eye Surgery PDFCod Mobile100% (1)
- Congenital Strabismus: S. Vanitha, B.optom, 3 YearDokument23 SeitenCongenital Strabismus: S. Vanitha, B.optom, 3 YearDivya Priya Dharmalingam100% (1)
- 2008 - Irregular - Astigmatism - Diagnosis - (Ming - Wang - MD) - PDFDokument606 Seiten2008 - Irregular - Astigmatism - Diagnosis - (Ming - Wang - MD) - PDFRuslan IshalNoch keine Bewertungen
- Ocular EmergDokument61 SeitenOcular EmergKBR RS UNHAS100% (1)
- Perimetry-Reading A Sinsle FieldDokument69 SeitenPerimetry-Reading A Sinsle FieldMayank JainNoch keine Bewertungen
- Slit-Lamp Biomicroscopy Module 1.4 - FINALDokument136 SeitenSlit-Lamp Biomicroscopy Module 1.4 - FINALloris1978s100% (2)
- Clinical Procedures in Primary Eye Care-David Elliott - 158Dokument3 SeitenClinical Procedures in Primary Eye Care-David Elliott - 158Danielle SangalangNoch keine Bewertungen
- FC Ophth (SA) Primary IA Past Papers - 2019 1st Semester 18-3-2019Dokument2 SeitenFC Ophth (SA) Primary IA Past Papers - 2019 1st Semester 18-3-2019Richard100% (1)
- Visual Field TestingDokument16 SeitenVisual Field TestingHendry HuangNoch keine Bewertungen
- DR Paul Krawitz - Ultimate Insiders Guide To Eye HealthDokument60 SeitenDR Paul Krawitz - Ultimate Insiders Guide To Eye HealthPro ANoch keine Bewertungen
- Posterior Polar Cataract Management: My Approach: 2022, #1Von EverandPosterior Polar Cataract Management: My Approach: 2022, #1Noch keine Bewertungen
- AutomatedPerimetry 2006Dokument208 SeitenAutomatedPerimetry 2006David ToddNoch keine Bewertungen
- Overview of Ophthalmic EquipmentDokument57 SeitenOverview of Ophthalmic EquipmenttallrajNoch keine Bewertungen
- Fundus ExaminationDokument43 SeitenFundus Examinationsamuelpnrj25100% (2)
- Direct OphthalmoscopeDokument16 SeitenDirect OphthalmoscopeMuhammed AbdulmajeedNoch keine Bewertungen
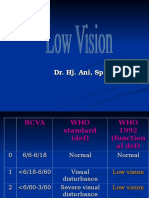
- Low VisionDokument36 SeitenLow VisionIqbal HabibieNoch keine Bewertungen
- Astigmatism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandAstigmatism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Cornea PDFDokument465 SeitenCornea PDFputraNoch keine Bewertungen
- Manual of Squint-Leela Ahuja - 48Dokument19 SeitenManual of Squint-Leela Ahuja - 48Danielle Sangalang100% (1)
- LASIK: A Guide to Laser Vision CorrectionVon EverandLASIK: A Guide to Laser Vision CorrectionBewertung: 2.5 von 5 Sternen2.5/5 (2)
- PhacoemulsificationDokument54 SeitenPhacoemulsificationIshita Kinra100% (1)
- Angle Closure Glaucoma PDFDokument289 SeitenAngle Closure Glaucoma PDFsisil muntheNoch keine Bewertungen
- Okap Samson Uveitis PDFDokument12 SeitenOkap Samson Uveitis PDFsharu4291Noch keine Bewertungen
- Glaucoma and Ocular HypertensionDokument6 SeitenGlaucoma and Ocular HypertensionsoniasistNoch keine Bewertungen
- Imaging of OrbitDokument69 SeitenImaging of OrbitFaisal ShembeshNoch keine Bewertungen
- Far-Sightedness, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandFar-Sightedness, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Night MiopiaDokument8 SeitenNight MiopiamurilobsouzaNoch keine Bewertungen
- Contact Lenses: Dr. Anupama Janardhanan Dr. Reji ThomasDokument107 SeitenContact Lenses: Dr. Anupama Janardhanan Dr. Reji ThomasAnupama Janardhanan100% (1)
- Eyelid AnatomyDokument66 SeitenEyelid AnatomyAnupama JanardhananNoch keine Bewertungen
- Pride and Honour: DR Anupama JanardhananDokument1 SeitePride and Honour: DR Anupama JanardhananAnupama JanardhananNoch keine Bewertungen
- Slit LampDokument84 SeitenSlit LampAnupama Janardhanan67% (3)
- Pandit Ravi Shankar-Dr Nalini JDokument3 SeitenPandit Ravi Shankar-Dr Nalini JAnupama JanardhananNoch keine Bewertungen
- Ghulam Ali-The Ustad of Ghazals-Dr - Major Nalini JanardhananDokument7 SeitenGhulam Ali-The Ustad of Ghazals-Dr - Major Nalini JanardhananAnupama JanardhananNoch keine Bewertungen
- RADHAMADHAVAN A Saga of Love and PainDokument3 SeitenRADHAMADHAVAN A Saga of Love and PainAnupama JanardhananNoch keine Bewertungen
- 12 Phy Pract Cbse FinalDokument66 Seiten12 Phy Pract Cbse Finalvelu NavaratnamNoch keine Bewertungen
- An FDTD Analysis of Nonlinear Photonic Crystal WavDokument13 SeitenAn FDTD Analysis of Nonlinear Photonic Crystal WavyassinebouazziNoch keine Bewertungen
- Masina de Masurat 3D PDFDokument40 SeitenMasina de Masurat 3D PDFIoana TriscaNoch keine Bewertungen
- Types of LightingDokument6 SeitenTypes of LightingJeremy AgustinNoch keine Bewertungen
- Online Application-Photograph Capturing GuidelinesDokument4 SeitenOnline Application-Photograph Capturing GuidelinesMuhammad Irfan ButtNoch keine Bewertungen
- Rectangular Glass Slab JenilDokument22 SeitenRectangular Glass Slab JenilJenis PatelNoch keine Bewertungen
- Price ListDokument16 SeitenPrice ListRajasekhar NannapaneniNoch keine Bewertungen
- Light Notes 1Dokument31 SeitenLight Notes 1api-233194737Noch keine Bewertungen
- Rakesh 10330404 MTech ThesisDokument101 SeitenRakesh 10330404 MTech ThesisLuluNoch keine Bewertungen
- HB CLS6B FKWDokument11 SeitenHB CLS6B FKWkrishNoch keine Bewertungen
- Frensel Lenses - Fresnel Technologies, IncDokument12 SeitenFrensel Lenses - Fresnel Technologies, IncBruce VanceNoch keine Bewertungen
- Light: Chapter 5 Year 4 (KSSR) Chapter 6 Year 5 (KBSR)Dokument11 SeitenLight: Chapter 5 Year 4 (KSSR) Chapter 6 Year 5 (KBSR)Subba KanesenNoch keine Bewertungen
- Non-Invasive Continuous Glucose MonitoringDokument7 SeitenNon-Invasive Continuous Glucose MonitoringLevente BalázsNoch keine Bewertungen
- Chapter 22.1 4Dokument34 SeitenChapter 22.1 4Richard Renz VillafuerteNoch keine Bewertungen
- Kuliah 6 - Biaxial FiguresDokument54 SeitenKuliah 6 - Biaxial FiguresBERNARDUS ANGGIT WINAHYUNoch keine Bewertungen
- Fact-Sheet-No.-19-Dec-2018 LASER WELDING AND CUTTING SAFETYDokument3 SeitenFact-Sheet-No.-19-Dec-2018 LASER WELDING AND CUTTING SAFETYCarlos BustamanteNoch keine Bewertungen
- Psfs and Sampling of Images in AstronomyDokument4 SeitenPsfs and Sampling of Images in AstronomyThilliNoch keine Bewertungen
- LED TestingDokument22 SeitenLED TestingSaket JhaNoch keine Bewertungen
- Method of Edge Waves in The Physical Theory of DiffractionDokument241 SeitenMethod of Edge Waves in The Physical Theory of DiffractionSatadal GuptaNoch keine Bewertungen
- Reference Guide To Fiber Optics: The Fiber Optic Association, IncDokument2 SeitenReference Guide To Fiber Optics: The Fiber Optic Association, IncShantanu BiswasNoch keine Bewertungen
- Polarizer: Linear PolarizersDokument11 SeitenPolarizer: Linear PolarizersOTTO_Noch keine Bewertungen
- Earlier in Lesson 3: Mirror Equation Magnification EquationDokument6 SeitenEarlier in Lesson 3: Mirror Equation Magnification EquationJisha KuruvillaNoch keine Bewertungen
- SOP To Provide The Procedure For Performance Verification and Maintenance of PDA and Spectrofluorometric Detectors. - SOP's For BA - BE StudiesDokument6 SeitenSOP To Provide The Procedure For Performance Verification and Maintenance of PDA and Spectrofluorometric Detectors. - SOP's For BA - BE Studiesblack moon funNoch keine Bewertungen
- O. Naumenko Et Al - Cavity Ring-Down Spectroscopy of H2 17-O in The Range 16570-17125 CM - 1Dokument7 SeitenO. Naumenko Et Al - Cavity Ring-Down Spectroscopy of H2 17-O in The Range 16570-17125 CM - 14534567Noch keine Bewertungen
- Chapter 14 - Electromagnetic Wave PropagationDokument8 SeitenChapter 14 - Electromagnetic Wave PropagationJames Bonafe100% (1)
- Ace Ds Ot VSP SM G657a2 v02 eDokument1 SeiteAce Ds Ot VSP SM G657a2 v02 eU San AungNoch keine Bewertungen
- HW 02 SolutionsDokument16 SeitenHW 02 SolutionsLuis Gutierrez MelgarejoNoch keine Bewertungen
- Color Blindness, OR Color Vision DeficienciesDokument11 SeitenColor Blindness, OR Color Vision DeficienciesSalih AliNoch keine Bewertungen
- Altair 105 Rumak Maksutov Review Astronomy Now Magazine 2010Dokument3 SeitenAltair 105 Rumak Maksutov Review Astronomy Now Magazine 2010Bartek LigockiNoch keine Bewertungen
- Bitumen of JudeaDokument2 SeitenBitumen of JudeaforonideoNoch keine Bewertungen