Das könnte Ihnen auch gefallen
- Pathophysiology of Chronic Renal FailureDokument4 SeitenPathophysiology of Chronic Renal FailureMalvinder Singh DhillonNoch keine Bewertungen
- Nerve PDFDokument30 SeitenNerve PDFMalvinder Singh DhillonNoch keine Bewertungen
- Nerve PDFDokument30 SeitenNerve PDFMalvinder Singh DhillonNoch keine Bewertungen
- 2017.06.03 4 BSAC 2017 SERVIN F. Pharmacology of Intravenous Induction Agents 1Dokument30 Seiten2017.06.03 4 BSAC 2017 SERVIN F. Pharmacology of Intravenous Induction Agents 1Malvinder Singh DhillonNoch keine Bewertungen
- Intravenous Anaesthetic Agents ExplainedDokument5 SeitenIntravenous Anaesthetic Agents ExplainedAlisya NadhilahNoch keine Bewertungen
- Peripheral Nerve Injuries - Suhaida-2Dokument79 SeitenPeripheral Nerve Injuries - Suhaida-2Malvinder Singh DhillonNoch keine Bewertungen
- The Ortho PodDokument60 SeitenThe Ortho PodxyequusNoch keine Bewertungen
- Advanced Clinical RotationDokument50 SeitenAdvanced Clinical Rotationsaphena parvaNoch keine Bewertungen
- Peripheral Nerve ExaminationDokument30 SeitenPeripheral Nerve ExaminationMalvinder Singh DhillonNoch keine Bewertungen
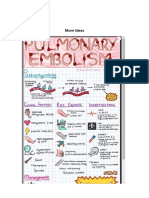
- More IdeasDokument1 SeiteMore IdeasMalvinder Singh DhillonNoch keine Bewertungen
- 227 Perioperative Renal DysfunctionDokument9 Seiten227 Perioperative Renal DysfunctionJuan LuisNoch keine Bewertungen
- 107 - IV Induction Agents PDFDokument17 Seiten107 - IV Induction Agents PDFTony AbottNoch keine Bewertungen
- Brachial Plexus ExaminationDokument7 SeitenBrachial Plexus ExaminationMalvinder Singh DhillonNoch keine Bewertungen
- MCQ SurgeryDokument17 SeitenMCQ SurgeryMalvinder Singh Dhillon50% (2)
- SURGICAL PROCEDURES AND DEVICES: CATHETERS, TUBES, STOMADokument5 SeitenSURGICAL PROCEDURES AND DEVICES: CATHETERS, TUBES, STOMAMalvinder Singh DhillonNoch keine Bewertungen
- Surgery InstrumentsDokument16 SeitenSurgery InstrumentsMalvinder Singh DhillonNoch keine Bewertungen
- Instrument Indentification in The Ward 1. Nasal Prong/ Nasal CannulaDokument14 SeitenInstrument Indentification in The Ward 1. Nasal Prong/ Nasal CannulaMalvinder Singh DhillonNoch keine Bewertungen
- O&G QuestionDokument6 SeitenO&G QuestionMalvinder Singh DhillonNoch keine Bewertungen
- Year 3 - Learning OutcomeDokument8 SeitenYear 3 - Learning OutcomeKalichandren ArumugamNoch keine Bewertungen
- History and ExaminationDokument45 SeitenHistory and ExaminationSerious SoNoch keine Bewertungen
- !THe H Book For 5th Year OSCE - Part 1 PDFDokument147 Seiten!THe H Book For 5th Year OSCE - Part 1 PDFMalvinder Singh DhillonNoch keine Bewertungen
- MEQ Pro 3 March 2016Dokument8 SeitenMEQ Pro 3 March 2016Malvinder Singh DhillonNoch keine Bewertungen
- Anatomy MnemonicsDokument4 SeitenAnatomy Mnemonicskiara91% (56)
- Surgical Drains Catheters and Tubes (M)Dokument120 SeitenSurgical Drains Catheters and Tubes (M)nikprov100% (6)
- Physical ExamDokument6 SeitenPhysical ExamTroy SilverioNoch keine Bewertungen
- Stroke Hosp PDFDokument1 SeiteStroke Hosp PDFMalvinder Singh DhillonNoch keine Bewertungen
- Fetal Health PDFDokument6 SeitenFetal Health PDFMalvinder Singh DhillonNoch keine Bewertungen
- Cardiac Arrest Pea and Asystole PDFDokument1 SeiteCardiac Arrest Pea and Asystole PDFMalvinder Singh DhillonNoch keine Bewertungen
- Adult Bls PDFDokument1 SeiteAdult Bls PDFMalvinder Singh DhillonNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Two Dimensional and M-Mode Echocardiography - BoonDokument112 SeitenTwo Dimensional and M-Mode Echocardiography - BoonRobles RobertoNoch keine Bewertungen
- Advance Trauma & Cardiovascular Life Support: Siswa Susdokbangan A-18Dokument86 SeitenAdvance Trauma & Cardiovascular Life Support: Siswa Susdokbangan A-18sahidakn100% (1)
- Nursing Care Plan - Myocardial InfarctionDokument3 SeitenNursing Care Plan - Myocardial Infarctionderic80% (10)
- Nclex ExamDokument164 SeitenNclex ExamZara Andrei100% (17)
- External Anatomy of The HeartDokument2 SeitenExternal Anatomy of The HeartAndres LarrottaNoch keine Bewertungen
- Basic Life Support (BLS) : Franklin O. Que, BSN-RNDokument90 SeitenBasic Life Support (BLS) : Franklin O. Que, BSN-RNfrank_1785Noch keine Bewertungen
- Cor Pulmonale PresentationDokument17 SeitenCor Pulmonale Presentationandi reskifaisNoch keine Bewertungen
- Clinical Cardiology - April 1994 - Wareing - Cardiac Surgery 2nd Edition by John W Kirklin and Brian G Barratt BoyesDokument1 SeiteClinical Cardiology - April 1994 - Wareing - Cardiac Surgery 2nd Edition by John W Kirklin and Brian G Barratt BoyesOlga KochubeiNoch keine Bewertungen
- Drug-Eluting Balloon: New Tool in The BoxDokument8 SeitenDrug-Eluting Balloon: New Tool in The BoxARUN KUMARNoch keine Bewertungen
- Cardiovascular SystemDokument6 SeitenCardiovascular Systemjamielsomera120Noch keine Bewertungen
- CatheterizationDokument2 SeitenCatheterizationElishah CaprichoNoch keine Bewertungen
- Maternal Early Warning System Proposed by National PartnershipDokument3 SeitenMaternal Early Warning System Proposed by National PartnershipDesi WildayaniNoch keine Bewertungen
- AHA Guidelines For CPR and ECC Comparison Chart of Key Changes (2010)Dokument8 SeitenAHA Guidelines For CPR and ECC Comparison Chart of Key Changes (2010)PhilippineNursingDirectory.comNoch keine Bewertungen
- Diagnosing Heart Failure with Preserved Ejection FractionDokument8 SeitenDiagnosing Heart Failure with Preserved Ejection FractionErwin GuerreroNoch keine Bewertungen
- Laporan Kasus - Dendy Dwi Ramadhani - PPDS Anestesi BrawijayaDokument1 SeiteLaporan Kasus - Dendy Dwi Ramadhani - PPDS Anestesi BrawijayaDendyNoch keine Bewertungen
- Aachen Resonance BiotronikDokument2 SeitenAachen Resonance BiotronikAlexander Ruebben100% (2)
- Aortic StenosisDokument11 SeitenAortic StenosisIra AnuddinNoch keine Bewertungen
- Nursing Care of Children with Cardiovascular DisordersDokument11 SeitenNursing Care of Children with Cardiovascular DisordersJœnríčk AzueloNoch keine Bewertungen
- CAB-CPR UpdateDokument15 SeitenCAB-CPR Updatedragon66Noch keine Bewertungen
- Advances in Electrocardiograms - Clinical Applns. - R. Millis (Intech, 2011) WW PDFDokument340 SeitenAdvances in Electrocardiograms - Clinical Applns. - R. Millis (Intech, 2011) WW PDFLisa BobulaNoch keine Bewertungen
- IHDW GuidelinesDokument32 SeitenIHDW GuidelinesCezara ZahariaNoch keine Bewertungen
- Management of CRAODokument3 SeitenManagement of CRAOvennieNoch keine Bewertungen
- Aortic Valve Stenosis Causes Left Ventricle FailureDokument30 SeitenAortic Valve Stenosis Causes Left Ventricle Failureloknath reddyNoch keine Bewertungen
- Heart Block PPT by SibaDokument36 SeitenHeart Block PPT by Sibaritumitu_ritumitu100% (1)
- 7 Pulmonary EdemaDokument10 Seiten7 Pulmonary Edemaomar kmr97Noch keine Bewertungen
- Ecg - Partea I - Mircea CintezaDokument16 SeitenEcg - Partea I - Mircea CintezaAndrei CiobotaruNoch keine Bewertungen
- Cardiovascular SystemDokument3 SeitenCardiovascular Systemhz1588Noch keine Bewertungen
- Nursing Management of a Patient with Kawasaki DiseaseDokument49 SeitenNursing Management of a Patient with Kawasaki DiseaseJemimah Ruth Madayag ValenzuelaNoch keine Bewertungen
- VerapamilDokument2 SeitenVerapamilMyla Reyes San MiguelNoch keine Bewertungen
- Cardiovascular SystemDokument6 SeitenCardiovascular Systemtasneem8Noch keine Bewertungen