Das könnte Ihnen auch gefallen
- Neonatal Emergencies (After Discharge) : Robert Englert, M.D. Dept Neonatology Bethesda Naval HospitalDokument43 SeitenNeonatal Emergencies (After Discharge) : Robert Englert, M.D. Dept Neonatology Bethesda Naval HospitalTresno JoyoNoch keine Bewertungen
- Alert Medical Series: Emergency Medicine Alert I, II, IIIVon EverandAlert Medical Series: Emergency Medicine Alert I, II, IIINoch keine Bewertungen
- Thomas R. Burklow, MD Asst C., Pediatric Cardiology Walter Reed Army Medical Center National Capital ConsortiumDokument40 SeitenThomas R. Burklow, MD Asst C., Pediatric Cardiology Walter Reed Army Medical Center National Capital ConsortiumMuna ZahiraNoch keine Bewertungen
- Acute and Chronic HepatitisDokument72 SeitenAcute and Chronic HepatitisArun George100% (3)
- 5 Asphyxia NeonetrumDokument27 Seiten5 Asphyxia NeonetrumRana VandanaNoch keine Bewertungen
- Pyloric StenosisDokument23 SeitenPyloric StenosisRama ItachiNoch keine Bewertungen
- Pediatric Renal & Genitourinary DisordersDokument72 SeitenPediatric Renal & Genitourinary DisordersMarie Angelique Cruz CrestaniNoch keine Bewertungen
- Pediatric Heart FailureDokument16 SeitenPediatric Heart FailureCharlie LeeNoch keine Bewertungen
- Perinatal Asphyxia: Walter Otieno Consultant PaediatricianDokument25 SeitenPerinatal Asphyxia: Walter Otieno Consultant PaediatricianMalueth AnguiNoch keine Bewertungen
- c1fd6bbd Ff7a 480d A20e C93bd3a3cedfDokument35 Seitenc1fd6bbd Ff7a 480d A20e C93bd3a3cedfapi-26938624Noch keine Bewertungen
- Birth AsphyxiaDokument26 SeitenBirth Asphyxiawizborrlyzo006Noch keine Bewertungen
- Review On Birth Asphyxia by TibinDokument22 SeitenReview On Birth Asphyxia by Tibintibinj67Noch keine Bewertungen
- 4 Ps NotesDokument33 Seiten4 Ps NotesErika Bea PaculanangNoch keine Bewertungen
- Hypertensive Disorders in PregnancyDokument81 SeitenHypertensive Disorders in PregnancyarunshreerajendranNoch keine Bewertungen
- Case Files PedsDokument54 SeitenCase Files PedsSam ZeezNoch keine Bewertungen
- Curs AsfixiaDokument15 SeitenCurs Asfixiamin09hihiNoch keine Bewertungen
- Acute Liver FailureDokument69 SeitenAcute Liver FailureAsif.N.IqbalNoch keine Bewertungen
- OBPreg NotesDokument7 SeitenOBPreg NotesfortitudemNoch keine Bewertungen
- Case Presentation On Pre-EclampsiaDokument18 SeitenCase Presentation On Pre-EclampsiaPabhat Kumar86% (7)
- Hypertensive Disorders of Pregnancy PDFDokument9 SeitenHypertensive Disorders of Pregnancy PDFMohammed AbdNoch keine Bewertungen
- MaeDokument9 SeitenMaeCharmaigne Mae Padilla Sotelo100% (1)
- Gestational HypertensionDokument10 SeitenGestational Hypertensionguptaavni0000Noch keine Bewertungen
- Preeclampsia and EclampsiaDokument24 SeitenPreeclampsia and EclampsiaFawzia Haznah Nurul ImaniNoch keine Bewertungen
- Hypertension in PregnancyDokument68 SeitenHypertension in PregnancyAbdul MoizNoch keine Bewertungen
- Pediatrics RemarksDokument62 SeitenPediatrics RemarksGÖKSU SAYGILINoch keine Bewertungen
- Pregnancy Induced Hypertension and Anesthesia Consideration: DR Asgher Niazi PGR-II AnesthesiaDokument45 SeitenPregnancy Induced Hypertension and Anesthesia Consideration: DR Asgher Niazi PGR-II AnesthesiaAsgher Khan NiaziNoch keine Bewertungen
- Perinatal Asphyxia: Presenters: Patrick Peter BwalyaDokument37 SeitenPerinatal Asphyxia: Presenters: Patrick Peter BwalyaHomeground entertainmentNoch keine Bewertungen
- Acute Liver Failure in PediatricDokument28 SeitenAcute Liver Failure in PediatricLillada Giftie AnuntarumpornNoch keine Bewertungen
- PediaDokument9 SeitenPediaFreema FloresNoch keine Bewertungen
- Hypertensive Disorders in PregnancyDokument40 SeitenHypertensive Disorders in PregnancyEzz Aldeen Bani Yaseen100% (1)
- Primary SurveyDokument13 SeitenPrimary SurveyNurul FadliNoch keine Bewertungen
- Endocrinology Teaching CasesDokument47 SeitenEndocrinology Teaching CasesBinta BaptisteNoch keine Bewertungen
- Fluid and Electrolyte 10 RDokument87 SeitenFluid and Electrolyte 10 RHea YaNoch keine Bewertungen
- Pre Anaesthetic Evaluation and Preparation of Children ForDokument48 SeitenPre Anaesthetic Evaluation and Preparation of Children ForMelvin CyriacNoch keine Bewertungen
- DR Mark Finney - HTN in Pregnancy MFAGDokument64 SeitenDR Mark Finney - HTN in Pregnancy MFAGPetros Akin-NibosunNoch keine Bewertungen
- Acute Liver Failure in ChildrenDokument34 SeitenAcute Liver Failure in ChildrenEpahNoch keine Bewertungen
- Peb InggrisDokument8 SeitenPeb InggrisRangga SaputraNoch keine Bewertungen
- Common Newborn Problems (2) C1Dokument39 SeitenCommon Newborn Problems (2) C1ZmNoch keine Bewertungen
- Hypertensive Disorders in PregnancyDokument27 SeitenHypertensive Disorders in PregnancyHarleyquinn96 DrNoch keine Bewertungen
- AnemiaDokument13 SeitenAnemiaguptaavni0000Noch keine Bewertungen
- Preeclampsia and EclampsiaDokument23 SeitenPreeclampsia and Eclampsiaapi-3705046100% (6)
- Severe Hypertension in PregnancyDokument31 SeitenSevere Hypertension in PregnancyHillio KuNoch keine Bewertungen
- RA 9288 Newborn Screening ActDokument40 SeitenRA 9288 Newborn Screening ActAkasha Frostmourne100% (2)
- Preeclampsia and EclampsiaDokument24 SeitenPreeclampsia and EclampsiaAngel Marie TeNoch keine Bewertungen
- Introduction To Congestive Heart Failure Diagnosis, Classifications & ManagementDokument50 SeitenIntroduction To Congestive Heart Failure Diagnosis, Classifications & Managementmadimadi11Noch keine Bewertungen
- Pediatric HandbookDokument201 SeitenPediatric HandbookJoseph MensaNoch keine Bewertungen
- Pre Eclampsia Nursing Care Plan by Maria Amabelles SorianoDokument39 SeitenPre Eclampsia Nursing Care Plan by Maria Amabelles SorianoLei Santillan0% (1)
- Hyperemesis Gravidarum AnemiaDokument10 SeitenHyperemesis Gravidarum AnemiaKate SantosNoch keine Bewertungen
- Thornton 2016Dokument5 SeitenThornton 2016AfdhalRuslanNoch keine Bewertungen
- Fulminant Hepatic Failure: Nattaphol UransilpDokument27 SeitenFulminant Hepatic Failure: Nattaphol UransilpChacha TasyaNoch keine Bewertungen
- Obstetrics Cases by Caroline de CostaDokument9 SeitenObstetrics Cases by Caroline de CostaJeffrey HingNoch keine Bewertungen
- Preeclampsia and EclampsiaDokument24 SeitenPreeclampsia and EclampsiaLuisa SarangayNoch keine Bewertungen
- Week 5 LectureDokument16 SeitenWeek 5 LectureMorgan LongworthNoch keine Bewertungen
- Preeclampsia & EclampsiaDokument24 SeitenPreeclampsia & EclampsiaIrfandy Chairi Sulaiman LubisNoch keine Bewertungen
- Birth Asphyxia: Walter Otieno Consultant PaediatricianDokument21 SeitenBirth Asphyxia: Walter Otieno Consultant PaediatricianMalueth AnguiNoch keine Bewertungen
- Hypertension in Pregnancy: Margaret S. Hamilton, DNS, RNDokument33 SeitenHypertension in Pregnancy: Margaret S. Hamilton, DNS, RNHaji RajiNoch keine Bewertungen
- Hypertensive Disorders in Pregnancy: Dr. Johanes C. Mose, DR, SpogDokument39 SeitenHypertensive Disorders in Pregnancy: Dr. Johanes C. Mose, DR, SpogfiskaNoch keine Bewertungen
- Morning Report Case Presentation: APRIL 1, 2019Dokument14 SeitenMorning Report Case Presentation: APRIL 1, 2019Emily EresumaNoch keine Bewertungen
- Pregnancy Induced HypertensionDokument52 SeitenPregnancy Induced HypertensionJoy GloryNoch keine Bewertungen
- Pengaruh Bauran Pemasaran Terhadap Jumlah Pasien Klinik Healthy LifeDokument1 SeitePengaruh Bauran Pemasaran Terhadap Jumlah Pasien Klinik Healthy LifeDennyNoch keine Bewertungen
- Parade Onko 1 Jan 3 JanDokument6 SeitenParade Onko 1 Jan 3 JanDennyNoch keine Bewertungen
- Understanding The Inflammatory Cytokine Response in Pneumonia and SepsisDokument9 SeitenUnderstanding The Inflammatory Cytokine Response in Pneumonia and SepsisDennyNoch keine Bewertungen
- Explore: NotesDokument20 SeitenExplore: NotesDennyNoch keine Bewertungen
- Echo LaliaDokument6 SeitenEcho LaliaDennyNoch keine Bewertungen
- HNPDokument7 SeitenHNPDennyNoch keine Bewertungen
- Morning Report 18 Febr 2015Dokument12 SeitenMorning Report 18 Febr 2015DennyNoch keine Bewertungen
- Status NeurologisDokument1 SeiteStatus NeurologisDennyNoch keine Bewertungen
- Cory Ne BacteriumDokument25 SeitenCory Ne BacteriumSona SandiNoch keine Bewertungen
- NDR KDokument61 SeitenNDR KВерка ПавловићNoch keine Bewertungen
- Keyword Ideas On Hair Loss For SEODokument18 SeitenKeyword Ideas On Hair Loss For SEOChitrakarudu KalabhimaniNoch keine Bewertungen
- Nervous System Concept MapDokument12 SeitenNervous System Concept MapJo BrackenNoch keine Bewertungen
- Farm Case StudyDokument10 SeitenFarm Case StudyAnthony WhelanNoch keine Bewertungen
- 5 6057344157398073400Dokument69 Seiten5 6057344157398073400Desmiyati AdoeNoch keine Bewertungen
- Noble Conflict by Malorie Blackman (Extract)Dokument13 SeitenNoble Conflict by Malorie Blackman (Extract)RandomHouse ChildrensPublishers0% (1)
- Resolving Negative Life ExperiencesDokument19 SeitenResolving Negative Life ExperiencessoriboNoch keine Bewertungen
- Anatomy and Physiology PDFDokument51 SeitenAnatomy and Physiology PDFalexenneth canilaNoch keine Bewertungen
- CBD DR Saugi IrfanDokument88 SeitenCBD DR Saugi IrfanFebri BimayanaNoch keine Bewertungen
- AGGIE Board ReviwerDokument43 SeitenAGGIE Board ReviwerQuinnee Vallejos100% (2)
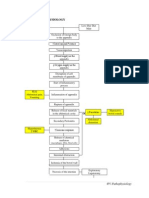
- Appendicitis PathophysiologyDokument4 SeitenAppendicitis PathophysiologyAngelica Cassandra VillenaNoch keine Bewertungen
- Theory Spleen and LiverDokument65 SeitenTheory Spleen and LiverMiddioPNoch keine Bewertungen
- Sanum Therapy Book Helios PDFDokument314 SeitenSanum Therapy Book Helios PDFOscarNoch keine Bewertungen
- National O.O. Bohomolets Medical University: Orthodontics and Prosthodontics Propedeutics DepartmentDokument63 SeitenNational O.O. Bohomolets Medical University: Orthodontics and Prosthodontics Propedeutics Departmentسینا ایرانیNoch keine Bewertungen
- Anatomy and Physiology of NoseDokument32 SeitenAnatomy and Physiology of NoseBinita ShakyaNoch keine Bewertungen
- Leadfinger GoblinDokument1 SeiteLeadfinger GoblinBrianNoch keine Bewertungen
- CurosurDokument2 SeitenCurosuredNoch keine Bewertungen
- IndomethacinDokument17 SeitenIndomethacinRajpal Singh KochharNoch keine Bewertungen
- MonstersandtreasureofaihrdeccDokument210 SeitenMonstersandtreasureofaihrdeccDaveDM100% (1)
- Reflexology On FootDokument16 SeitenReflexology On FootManish Anand100% (1)
- Bites and Stings - Dermatology - MKSAP 17Dokument4 SeitenBites and Stings - Dermatology - MKSAP 17Ciara Marjorie HannaNoch keine Bewertungen
- 15-10-2019, Mr. Jamal, 50 Yo, V.Laceratum Cruris Dextra + Skin Loss + Fraktur Os Fibula, Dr. Moh. Rizal Alizi, M.Kes, Sp. OT-1Dokument15 Seiten15-10-2019, Mr. Jamal, 50 Yo, V.Laceratum Cruris Dextra + Skin Loss + Fraktur Os Fibula, Dr. Moh. Rizal Alizi, M.Kes, Sp. OT-1anon_893244902Noch keine Bewertungen
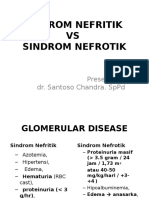
- Sindroma Nefrotik Vs NefritikDokument23 SeitenSindroma Nefrotik Vs NefritikihsanNoch keine Bewertungen
- Prevention of ThalassemiaDokument13 SeitenPrevention of Thalassemiavenka07Noch keine Bewertungen
- It Is Often Said That Government Spend Too Much Money On Projects To Protect WildlifeDokument1 SeiteIt Is Often Said That Government Spend Too Much Money On Projects To Protect WildlifeKaungPyae SoneNoch keine Bewertungen
- Comparision of Condylar Guidance Setting Obtained From A Wax Record Vs An Extra Oral TracingDokument6 SeitenComparision of Condylar Guidance Setting Obtained From A Wax Record Vs An Extra Oral TracingHarsha ReddyNoch keine Bewertungen
- Whybatsflyonlyatnight CLRDokument7 SeitenWhybatsflyonlyatnight CLRRaj ManoNoch keine Bewertungen
- Subcutaneous Infections and True PathogensDokument2 SeitenSubcutaneous Infections and True PathogensthescarletpimpernelsNoch keine Bewertungen
- Trial IGCSE (P1) 2022 - 2023Dokument16 SeitenTrial IGCSE (P1) 2022 - 2023Andrew PooleNoch keine Bewertungen