Das könnte Ihnen auch gefallen
- Cerebral PalsyDokument97 SeitenCerebral PalsyPrernaSharma100% (3)
- Cerebral Palsy: I. Definition/ DescriptionDokument4 SeitenCerebral Palsy: I. Definition/ Descriptionfaye kim100% (1)
- Cerebral PalsyDokument11 SeitenCerebral PalsySanthosh.S.UNoch keine Bewertungen
- Cerebral PalsyDokument25 SeitenCerebral PalsyTINTU JOSEPHNoch keine Bewertungen
- Case Based Pediatrics CEREBRAL PALSYDokument5 SeitenCase Based Pediatrics CEREBRAL PALSYNabighah ZukriNoch keine Bewertungen
- G & D Assessment, Growth ChartDokument12 SeitenG & D Assessment, Growth ChartThilaga RamNoch keine Bewertungen
- Cerebral PalsyDokument2 SeitenCerebral PalsyTracy100% (1)
- Muscular DystrophyDokument21 SeitenMuscular DystrophyIqra Iftikhar100% (4)
- Down SyndromeDokument29 SeitenDown SyndromeFatima yasin60% (5)
- Parkinson DiseaseDokument14 SeitenParkinson DiseasemulfasatriaNoch keine Bewertungen
- ClubfootDokument21 SeitenClubfootRoss Carolino Fernandez100% (1)
- Junevile DM Kel. 4Dokument7 SeitenJunevile DM Kel. 4suci arleniaNoch keine Bewertungen
- HydrocephalusDokument33 SeitenHydrocephalusrajan kumar100% (2)
- Club Foot (Congenital Talipes Equinovarus) Club Foot (Congenital Talipes Equinovarus)Dokument24 SeitenClub Foot (Congenital Talipes Equinovarus) Club Foot (Congenital Talipes Equinovarus)jyoti kunduNoch keine Bewertungen
- Down SyndromeDokument18 SeitenDown Syndromepreciouslacdan86% (7)
- Epilepsy - Case StudyDokument11 SeitenEpilepsy - Case StudyHarry Sivia100% (3)
- Milestone FinalDokument21 SeitenMilestone FinalFransric TinampayNoch keine Bewertungen
- Approach To Floppy InfantDokument44 SeitenApproach To Floppy InfantShauki AliNoch keine Bewertungen
- Newborn ReflexesDokument41 SeitenNewborn ReflexesUmairah Bashir100% (5)
- Review On Birth Asphyxia by TibinDokument22 SeitenReview On Birth Asphyxia by Tibintibinj67Noch keine Bewertungen
- High Risk New BornDokument36 SeitenHigh Risk New BornIze C VijiNoch keine Bewertungen
- Cerebral PalsyDokument21 SeitenCerebral PalsyEMily AbastaNoch keine Bewertungen
- Child - Cerebral PalsyDokument3 SeitenChild - Cerebral PalsyJamie Icabandi67% (3)
- My - Failure To ThriveDokument31 SeitenMy - Failure To ThriveAuliaRahman100% (1)
- Congenital AnomaliesDokument94 SeitenCongenital AnomaliesDeepti Kukreti100% (1)
- Role of Pediatric Nurse in Child CareDokument4 SeitenRole of Pediatric Nurse in Child CarevishnuNoch keine Bewertungen
- Cerebral Palsy AssessmentDokument8 SeitenCerebral Palsy Assessmentrajalaxmi gopalakrishnanNoch keine Bewertungen
- Bell - S PalsyDokument17 SeitenBell - S PalsyRickzen Hawkins NikecholantNoch keine Bewertungen
- Failure To Thrive (FTT)Dokument23 SeitenFailure To Thrive (FTT)Endrow Francisco100% (1)
- Spina BifidaDokument6 SeitenSpina BifidaAnn Remz100% (3)
- BEHAVIORAL PEDIatricsDokument119 SeitenBEHAVIORAL PEDIatricskrishnasree67% (3)
- Spina Bifida PresentationDokument11 SeitenSpina Bifida Presentationapi-242435091Noch keine Bewertungen
- Cerebral PalsyDokument33 SeitenCerebral Palsyvimal rajNoch keine Bewertungen
- HydrocephalusDokument21 SeitenHydrocephalusprecillathoppil100% (2)
- Pyloric StenosisDokument3 SeitenPyloric Stenosismagisasamundo100% (1)
- Cerebral Palsy AssessmentDokument6 SeitenCerebral Palsy AssessmentdrprasantNoch keine Bewertungen
- Down Syndrome (Case Presentation Output)Dokument6 SeitenDown Syndrome (Case Presentation Output)Jommel Ryan Corpus LumibaoNoch keine Bewertungen
- Muscle Tone and Reflex AssessmentDokument31 SeitenMuscle Tone and Reflex Assessmentenrico_aguila100% (3)
- Behavioural Problems in ChildrenDokument49 SeitenBehavioural Problems in ChildrenAshly Nygil100% (1)
- Introduction To Theories of Neurological RehabilitationDokument30 SeitenIntroduction To Theories of Neurological RehabilitationHibaAli67% (3)
- Definition, Etiology, Epidemiology of Down SyndromeDokument5 SeitenDefinition, Etiology, Epidemiology of Down Syndromedi_sooNoch keine Bewertungen
- Birth Asphyxia: Chinju Elsa ThomasDokument61 SeitenBirth Asphyxia: Chinju Elsa Thomaslumina.s100% (1)
- Organization of Neonatal Intensive Care Unit: Vanderbilt University Mildred Stahlman StahlmanDokument12 SeitenOrganization of Neonatal Intensive Care Unit: Vanderbilt University Mildred Stahlman StahlmanKiran Kumar100% (1)
- 1 To 4 Growth and DevelopmentDokument126 Seiten1 To 4 Growth and DevelopmentArchanaNoch keine Bewertungen
- Care of Preterm Babies FinalDokument33 SeitenCare of Preterm Babies Finalchinchu100% (1)
- Club FootDokument5 SeitenClub FootNika Joy Cabrera AlarconNoch keine Bewertungen
- Monitoring & Care of Ventilated ChildrenDokument12 SeitenMonitoring & Care of Ventilated ChildrenRajakumar Padur Sivaraman100% (2)
- Case Study SlideshowDokument48 SeitenCase Study Slideshowapi-3342471330% (1)
- Nursing Care of Children With BurnsDokument52 SeitenNursing Care of Children With Burnskarpagamanbu100% (5)
- Pediatric Nursing: Narayan Swami College of NursingDokument10 SeitenPediatric Nursing: Narayan Swami College of NursingAnkit KotnalaNoch keine Bewertungen
- Occupational TherapyDokument15 SeitenOccupational Therapymanu sethi100% (1)
- Cerebral Palsy Assessment ImportantDokument7 SeitenCerebral Palsy Assessment Importantabra_arr100% (2)
- EncephalitisDokument37 SeitenEncephalitisPRADEEPNoch keine Bewertungen
- Congenital Hip DislocationDokument6 SeitenCongenital Hip DislocationPaola CamainNoch keine Bewertungen
- New Born ReflexesDokument11 SeitenNew Born ReflexesBinal JoshiNoch keine Bewertungen
- Discuss Surgical Management of Cerebral Palsy - 000Dokument72 SeitenDiscuss Surgical Management of Cerebral Palsy - 000SamNoch keine Bewertungen
- Common Neonatal DisordersDokument70 SeitenCommon Neonatal DisordersKiran Khasa100% (4)
- Cerebral Palsy: I. Definition/ DescriptionDokument5 SeitenCerebral Palsy: I. Definition/ Descriptionfaye kimNoch keine Bewertungen
- Group 1Dokument35 SeitenGroup 1Fitri IsnainiNoch keine Bewertungen
- Cerebral Palsy 08.04.15 LectureDokument25 SeitenCerebral Palsy 08.04.15 LectureEmmanuel MukukaNoch keine Bewertungen
- Postpartum Hemorrhage FinalDokument6 SeitenPostpartum Hemorrhage Finalvarshasharma05Noch keine Bewertungen
- Lesson Plan On Collection of SpecimenDokument3 SeitenLesson Plan On Collection of Specimenvarshasharma0567% (3)
- Antenatal Care: Continuing Medical Education Activities For Non-Specialists DR TC Pun 27/2/2002Dokument84 SeitenAntenatal Care: Continuing Medical Education Activities For Non-Specialists DR TC Pun 27/2/2002tchale1Noch keine Bewertungen
- Female PelvisDokument4 SeitenFemale Pelvisvarshasharma05100% (1)
- Lesson Plan On Patterns of Nursing Education and Training Programmmes in IndiaDokument15 SeitenLesson Plan On Patterns of Nursing Education and Training Programmmes in Indiavarshasharma05Noch keine Bewertungen
- Allcandidates Nurse 2Dokument5.025 SeitenAllcandidates Nurse 2varshasharma050% (1)
- 3rd Stage of LabourDokument22 Seiten3rd Stage of Labourvarshasharma05100% (6)
- Training Module Qualitative Research UpdatedDokument4 SeitenTraining Module Qualitative Research Updatedvarshasharma05Noch keine Bewertungen
- Wa0001Dokument8 SeitenWa0001varshasharma05Noch keine Bewertungen
- Female PelvisDokument4 SeitenFemale Pelvisvarshasharma05100% (1)
- First Page PDFDokument1 SeiteFirst Page PDFvarshasharma05Noch keine Bewertungen
- Handouts On Research Problem StatementDokument2 SeitenHandouts On Research Problem Statementvarshasharma05100% (1)
- CommunicationDokument23 SeitenCommunicationvarshasharma05Noch keine Bewertungen
- Lesson Plan On Eclampsia: Submitted To Mrs. Cimil Babu Assistant Professor Holi Family College of NursingDokument13 SeitenLesson Plan On Eclampsia: Submitted To Mrs. Cimil Babu Assistant Professor Holi Family College of Nursingvarshasharma0580% (5)
- COVID-19 Prevention & IEC Committee, PGIMER Chandigarh: Tentative Webinar Schedule For Healthcare ProfessionalsDokument3 SeitenCOVID-19 Prevention & IEC Committee, PGIMER Chandigarh: Tentative Webinar Schedule For Healthcare Professionalsvarshasharma05Noch keine Bewertungen
- Post B BSC Unit PlanDokument3 SeitenPost B BSC Unit Planvarshasharma05100% (4)
- Midwife MeansDokument17 SeitenMidwife Meansvarshasharma05Noch keine Bewertungen
- Menstrual CycleDokument9 SeitenMenstrual Cyclevarshasharma05100% (2)
- 160 Nursing Bullets: Medical-Surgical Nursing Reviewer: Nursing Diagnosis Care Plan NCLEX Questions Exam QuestionDokument16 Seiten160 Nursing Bullets: Medical-Surgical Nursing Reviewer: Nursing Diagnosis Care Plan NCLEX Questions Exam Questionvarshasharma05100% (4)
- Lesson Plan On Eclampsia: Submitted To Mrs. Cimil Babu Assistant Professor Holi Family College of NursingDokument13 SeitenLesson Plan On Eclampsia: Submitted To Mrs. Cimil Babu Assistant Professor Holi Family College of Nursingvarshasharma0580% (5)
- Lesson Plan On PoliomyelitisDokument12 SeitenLesson Plan On Poliomyelitisvarshasharma05100% (1)
- Holy Family College of Nursing M.Sc. Nursing Second Year Obstetrics and Gynecology Master RotationDokument2 SeitenHoly Family College of Nursing M.Sc. Nursing Second Year Obstetrics and Gynecology Master Rotationvarshasharma05Noch keine Bewertungen
- 3rd Stage of Labour PDFDokument15 Seiten3rd Stage of Labour PDFvarshasharma05Noch keine Bewertungen
- Baby Friendly Hospital Initiative and Exclusive Breast FeedingDokument92 SeitenBaby Friendly Hospital Initiative and Exclusive Breast Feedingvarshasharma05Noch keine Bewertungen
- 3rd Stage of Labour PDFDokument15 Seiten3rd Stage of Labour PDFvarshasharma05Noch keine Bewertungen
- Notice No. 82 - NursingOfficerDokument8 SeitenNotice No. 82 - NursingOfficervarshasharma05Noch keine Bewertungen
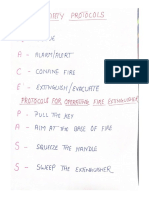
- Fire Safety ProtocolDokument1 SeiteFire Safety Protocolvarshasharma05Noch keine Bewertungen
- Care of Low Birth Weight BabiesDokument102 SeitenCare of Low Birth Weight Babiesvarshasharma05100% (1)
- Breastfeeding 120912050521 Phpapp01Dokument57 SeitenBreastfeeding 120912050521 Phpapp01varshasharma05Noch keine Bewertungen
- CareDokument18 SeitenCarevarshasharma05Noch keine Bewertungen
- The JHipster Mini Book 2Dokument129 SeitenThe JHipster Mini Book 2tyulist100% (1)
- Waterstop TechnologyDokument69 SeitenWaterstop TechnologygertjaniNoch keine Bewertungen
- Monergism Vs SynsergismDokument11 SeitenMonergism Vs SynsergismPam AgtotoNoch keine Bewertungen
- Harper Independent Distributor Tri FoldDokument2 SeitenHarper Independent Distributor Tri FoldYipper ShnipperNoch keine Bewertungen
- Report Card Grade 1 2Dokument3 SeitenReport Card Grade 1 2Mely DelacruzNoch keine Bewertungen
- Mcom Sem 4 Project FinalDokument70 SeitenMcom Sem 4 Project Finallaxmi iyer75% (4)
- Corrosion Fatigue Phenomena Learned From Failure AnalysisDokument10 SeitenCorrosion Fatigue Phenomena Learned From Failure AnalysisDavid Jose Velandia MunozNoch keine Bewertungen
- Fss Presentation Slide GoDokument13 SeitenFss Presentation Slide GoReinoso GreiskaNoch keine Bewertungen
- My Personal Code of Ethics1Dokument1 SeiteMy Personal Code of Ethics1Princess Angel LucanasNoch keine Bewertungen
- What Is TranslationDokument3 SeitenWhat Is TranslationSanskriti MehtaNoch keine Bewertungen
- PyhookDokument23 SeitenPyhooktuan tuanNoch keine Bewertungen
- School of Mathematics 2021 Semester 1 MAT1841 Continuous Mathematics For Computer Science Assignment 1Dokument2 SeitenSchool of Mathematics 2021 Semester 1 MAT1841 Continuous Mathematics For Computer Science Assignment 1STEM Education Vung TauNoch keine Bewertungen
- ME Eng 8 Q1 0101 - SG - African History and LiteratureDokument13 SeitenME Eng 8 Q1 0101 - SG - African History and Literaturerosary bersanoNoch keine Bewertungen
- in Strategic Management What Are The Problems With Maintaining A High Inventory As Experienced Previously With Apple?Dokument5 Seitenin Strategic Management What Are The Problems With Maintaining A High Inventory As Experienced Previously With Apple?Priyanka MurthyNoch keine Bewertungen
- Task 3 - LPDokument21 SeitenTask 3 - LPTan S YeeNoch keine Bewertungen
- LTE Networks Engineering Track Syllabus Overview - 23 - 24Dokument4 SeitenLTE Networks Engineering Track Syllabus Overview - 23 - 24Mohamed SamiNoch keine Bewertungen
- Mark Garside Resume May 2014Dokument3 SeitenMark Garside Resume May 2014api-199955558Noch keine Bewertungen
- Project - New Restuarant Management System The Grill HouseDokument24 SeitenProject - New Restuarant Management System The Grill HouseMayank Mahajan100% (3)
- IMS Objectives Targets 2Dokument2 SeitenIMS Objectives Targets 2FaridUddin Ahmed100% (3)
- Manual s10 PDFDokument402 SeitenManual s10 PDFLibros18Noch keine Bewertungen
- Technical Bulletin LXL: No. Subject Release DateDokument8 SeitenTechnical Bulletin LXL: No. Subject Release DateTrunggana AbdulNoch keine Bewertungen
- Chemistry Test 1Dokument2 SeitenChemistry Test 1shashankNoch keine Bewertungen
- 13 Adsorption of Congo Red A Basic Dye by ZnFe-CO3Dokument10 Seiten13 Adsorption of Congo Red A Basic Dye by ZnFe-CO3Jorellie PetalverNoch keine Bewertungen
- Wilcoxon Matched Pairs Signed Rank TestDokument3 SeitenWilcoxon Matched Pairs Signed Rank TestDawn Ilish Nicole DiezNoch keine Bewertungen
- Tribal Banditry in Ottoman Ayntab (1690-1730)Dokument191 SeitenTribal Banditry in Ottoman Ayntab (1690-1730)Mahir DemirNoch keine Bewertungen
- Lesson 6 ComprogDokument25 SeitenLesson 6 ComprogmarkvillaplazaNoch keine Bewertungen
- Oracle Forms & Reports 12.2.1.2.0 - Create and Configure On The OEL 7Dokument50 SeitenOracle Forms & Reports 12.2.1.2.0 - Create and Configure On The OEL 7Mario Vilchis Esquivel100% (1)
- Emea 119948060Dokument31 SeitenEmea 119948060ASHUTOSH MISHRANoch keine Bewertungen
- Traveling Salesman ProblemDokument11 SeitenTraveling Salesman ProblemdeardestinyNoch keine Bewertungen
- Arnold Ventures Letter To Congressional Social Determinants of Health CaucusDokument7 SeitenArnold Ventures Letter To Congressional Social Determinants of Health CaucusArnold VenturesNoch keine Bewertungen