Das könnte Ihnen auch gefallen
- The Circulatory SystemDokument53 SeitenThe Circulatory SystemVera June RañesesNoch keine Bewertungen
- Beating with Precision: The Science of Cardiology: Understand the Intricacies of the Human HeartVon EverandBeating with Precision: The Science of Cardiology: Understand the Intricacies of the Human HeartNoch keine Bewertungen
- Components of The Cardiovascular SystemDokument23 SeitenComponents of The Cardiovascular SystemMr. DummyNoch keine Bewertungen
- Cardiac PhysiologyDokument102 SeitenCardiac PhysiologyPeter Larsen100% (1)
- Cardiovascular and Circulatory SystemDokument29 SeitenCardiovascular and Circulatory SystemfayeleechaiyapornkulNoch keine Bewertungen
- CirculationDokument11 SeitenCirculationRishikaphriya RauichandranNoch keine Bewertungen
- Lesson 3Dokument71 SeitenLesson 3Angel joyce ValenciaNoch keine Bewertungen
- Regulation of Heart Rate, Stroke Volume, Cardiac Output, Blood FlowDokument20 SeitenRegulation of Heart Rate, Stroke Volume, Cardiac Output, Blood FlowShveta MahajanNoch keine Bewertungen
- Pathophysiology of Cardiovascular System Feghiu I., Tacu L., Iarovoi ADokument25 SeitenPathophysiology of Cardiovascular System Feghiu I., Tacu L., Iarovoi ALunguVictoriaNoch keine Bewertungen
- Cardiac CycleDokument3 SeitenCardiac CycleKhadijah HabeebahNoch keine Bewertungen
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Von EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Noch keine Bewertungen
- 2015A&PIntro CardiovascularHandoutDokument16 Seiten2015A&PIntro CardiovascularHandoutMaggieHameedNoch keine Bewertungen
- CHAPTER 35 Cardiac DisordersDokument93 SeitenCHAPTER 35 Cardiac DisordersIfy OhansonNoch keine Bewertungen
- Cardiovascular DrugsDokument33 SeitenCardiovascular DrugsKish Gabriel100% (1)
- Cardiovascular SystemDokument8 SeitenCardiovascular Systemomar farooqNoch keine Bewertungen
- الجهاز الدوريDokument16 Seitenالجهاز الدوريHUAWEI HUAWEINoch keine Bewertungen
- Visceral Vascular Manipulation, 2011Dokument270 SeitenVisceral Vascular Manipulation, 2011kkalu_just_funky91% (11)
- Cardiovascular Physiology: The Autonomic Nervous SystemDokument8 SeitenCardiovascular Physiology: The Autonomic Nervous SystemRidha Surya NugrahaNoch keine Bewertungen
- Circulation NotesDokument2 SeitenCirculation NotesBhkti MittalNoch keine Bewertungen
- Note On Pressure Flow and ResistanceDokument43 SeitenNote On Pressure Flow and ResistanceSilver FestusNoch keine Bewertungen
- Case 3Dokument4 SeitenCase 3the urvashiNoch keine Bewertungen
- WK 1& 2 LectureDokument149 SeitenWK 1& 2 LectureElma SekikorolevuNoch keine Bewertungen
- University of Goce Delcev StipDokument11 SeitenUniversity of Goce Delcev StipviktorijatalevskaNoch keine Bewertungen
- 565656Dokument61 Seiten565656Bashar AntriNoch keine Bewertungen
- Cardiovascularsystem 090820055728 Phpapp02Dokument75 SeitenCardiovascularsystem 090820055728 Phpapp02muhammad ijazNoch keine Bewertungen
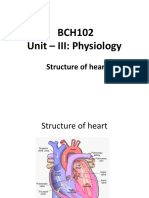
- BCH102 Unit - III: Physiology: Structure of HeartDokument17 SeitenBCH102 Unit - III: Physiology: Structure of Heartdivya vajpayeeNoch keine Bewertungen
- B1+ Student BookDokument60 SeitenB1+ Student BookKimsun DalinNoch keine Bewertungen
- Basic Principles of ECG InterpretationDokument26 SeitenBasic Principles of ECG Interpretationgosai83Noch keine Bewertungen
- Blood Circulatory SystemDokument8 SeitenBlood Circulatory SystemstephanietoppoNoch keine Bewertungen
- Cardiovascular System - Lecture IDokument4 SeitenCardiovascular System - Lecture IpragantraNoch keine Bewertungen
- Anatomy and Physiology of HeartDokument5 SeitenAnatomy and Physiology of HeartAmit MartinNoch keine Bewertungen
- Summary Vet Quiz (Cvs-Heart)Dokument3 SeitenSummary Vet Quiz (Cvs-Heart)Deeza Joice CastañedaNoch keine Bewertungen
- Session 5Dokument41 SeitenSession 5tazebNoch keine Bewertungen
- CV-5 PH MicrocircDokument34 SeitenCV-5 PH Microcircaya najemNoch keine Bewertungen
- Anatomi Fisiologi Sistem Kardiovaskuler 1Dokument52 SeitenAnatomi Fisiologi Sistem Kardiovaskuler 1Vaweli Putri Spelman DpNoch keine Bewertungen
- The Circulatory SystemDokument51 SeitenThe Circulatory SystemMohammed ahmedNoch keine Bewertungen
- Cardiovascular System: Presented by DR Aparna Ramachandran Mds 1 Dept of Public Health DentistryDokument73 SeitenCardiovascular System: Presented by DR Aparna Ramachandran Mds 1 Dept of Public Health DentistryAparna RamachandranNoch keine Bewertungen
- A&p (B&C) Handout 2015Dokument50 SeitenA&p (B&C) Handout 2015Alisa BrownNoch keine Bewertungen
- HeartDokument36 SeitenHeartSoovendran VaradarajanNoch keine Bewertungen
- Cardiovascular SystemDokument37 SeitenCardiovascular SystemHira KhanNoch keine Bewertungen
- Physiology of ExerciseDokument25 SeitenPhysiology of ExerciseTedy Friyadi100% (1)
- CardiovascularDokument36 SeitenCardiovascularShield Mae BalanlayNoch keine Bewertungen
- Diseases of The Heart Part 1Dokument141 SeitenDiseases of The Heart Part 1Amanuel MaruNoch keine Bewertungen
- SystemDokument63 SeitenSystemBeth Rubin RelatorNoch keine Bewertungen
- CV PathoDokument32 SeitenCV PathoSaif AliNoch keine Bewertungen
- Technical DefinitionDokument3 SeitenTechnical DefinitionErin BarnesNoch keine Bewertungen
- Electrocardiography (ECG)Dokument11 SeitenElectrocardiography (ECG)Hassan AnwarNoch keine Bewertungen
- Digital Heart Beat Counter: Project Report ONDokument76 SeitenDigital Heart Beat Counter: Project Report ONlkosumdecNoch keine Bewertungen
- EKG Study Guide RevisedDokument29 SeitenEKG Study Guide Revisedflashyboy506Noch keine Bewertungen
- Cardiovascular AssessmentDokument182 SeitenCardiovascular AssessmentAbie Jean BalbontinNoch keine Bewertungen
- Anatomia y Fisiologuia General Libro-851-900Dokument50 SeitenAnatomia y Fisiologuia General Libro-851-900Felipe Aguirre CórdovaNoch keine Bewertungen
- Special Regional CirculationDokument28 SeitenSpecial Regional CirculationBenjamin SharonNoch keine Bewertungen
- Chapter I - Cardiovascular System: HeartDokument2 SeitenChapter I - Cardiovascular System: HeartIndranil SinhaNoch keine Bewertungen
- Heart & Hemodynamics NotesDokument8 SeitenHeart & Hemodynamics NotesBrandice BradleyNoch keine Bewertungen
- Cardiovascular SystemDokument10 SeitenCardiovascular SystemDhea BugnaNoch keine Bewertungen
- Circulation and Cardiovascular SystemDokument12 SeitenCirculation and Cardiovascular SystemSatria MandalaNoch keine Bewertungen
- Cardiogenic ShockDokument14 SeitenCardiogenic ShockZellanien hdNoch keine Bewertungen
- Cardio Review Assignment-2Dokument2 SeitenCardio Review Assignment-2Sam VNoch keine Bewertungen
- ELEC4810 Notes-7 PDFDokument61 SeitenELEC4810 Notes-7 PDFKwan ChanNoch keine Bewertungen
- Introduction To BiostatisticsDokument73 SeitenIntroduction To BiostatisticsOrindia SuarminNoch keine Bewertungen
- Aerosol Delivery System: Tugas Sistem Penghantaran Obat Kelas A Kelompok 1Dokument33 SeitenAerosol Delivery System: Tugas Sistem Penghantaran Obat Kelas A Kelompok 1Orindia SuarminNoch keine Bewertungen
- Suhu 30 0C: F (X) - 0.01x + 50.07 R 0.97 LinearDokument5 SeitenSuhu 30 0C: F (X) - 0.01x + 50.07 R 0.97 LinearOrindia SuarminNoch keine Bewertungen
- DapusDokument11 SeitenDapusOrindia SuarminNoch keine Bewertungen
- CLASSIC ARTICLE Clinical Measurement and EvaluationDokument5 SeitenCLASSIC ARTICLE Clinical Measurement and EvaluationJesusCordoba100% (2)
- FISIOLOGI HAID-tgs DR NasDokument24 SeitenFISIOLOGI HAID-tgs DR NasShandy Suwanto PutraNoch keine Bewertungen
- CMR Guide CHD 2014 PDFDokument105 SeitenCMR Guide CHD 2014 PDFBasemAlharbiNoch keine Bewertungen
- Guruji 2Dokument176 SeitenGuruji 2Cine Dada67% (6)
- Key Elements of Animal Husbandry and Its Inspections: GMP Workshop For Inspection of Vaccines Manufacturing UnitsDokument26 SeitenKey Elements of Animal Husbandry and Its Inspections: GMP Workshop For Inspection of Vaccines Manufacturing UnitslanNoch keine Bewertungen
- Facts About Respiratory SystemDokument10 SeitenFacts About Respiratory SystemGermie Mariel GojarNoch keine Bewertungen
- Zoology HonsDokument80 SeitenZoology HonsSantosh MahathaNoch keine Bewertungen
- Bleeds Management-RICEhaemophiliaDokument1 SeiteBleeds Management-RICEhaemophiliaJohnnyNoch keine Bewertungen
- Human Rabies in The PhilippinesDokument2 SeitenHuman Rabies in The PhilippinesAngeli SoabasNoch keine Bewertungen
- 160 174+Pendampingan+Asuhan+Keperawatan+Medikal+Bedah+Pada+Pasien+Dengan+Gangguan+Sistem+Integument+ (Snake+Bite) +Di+Ruang+Anggrek+RSUD+BanjarDokument15 Seiten160 174+Pendampingan+Asuhan+Keperawatan+Medikal+Bedah+Pada+Pasien+Dengan+Gangguan+Sistem+Integument+ (Snake+Bite) +Di+Ruang+Anggrek+RSUD+BanjarRafli TarNoch keine Bewertungen
- Evaluation and Reduction of Nasal TraumaDokument15 SeitenEvaluation and Reduction of Nasal TraumaAnnisa Priscasari DwiyantiNoch keine Bewertungen
- ROSE Chapter 2Dokument19 SeitenROSE Chapter 2Gabriel PascualNoch keine Bewertungen
- AbdomenDokument1 SeiteAbdomenMonica SabarreNoch keine Bewertungen
- What The Doctor Needs To Know in Order To Make A Successful Prescription.Dokument45 SeitenWhat The Doctor Needs To Know in Order To Make A Successful Prescription.api-3708828100% (1)
- Fouchet's Test 3Dokument5 SeitenFouchet's Test 3david mchembeNoch keine Bewertungen
- Medical Exams - San SalvadorDokument6 SeitenMedical Exams - San SalvadorrodriguezsoulNoch keine Bewertungen
- 5th Grade Unit 5 Health Practice Makes Perfect! 1 Worksheet 1 PDFDokument2 Seiten5th Grade Unit 5 Health Practice Makes Perfect! 1 Worksheet 1 PDFAmin ZakiNoch keine Bewertungen
- Handp TemplateDokument3 SeitenHandp TemplateLauren GrandpreNoch keine Bewertungen
- Diagnose Cure and Empower Yourself by Currents of Breath - Authored by Acharya Shriram SharmaDokument78 SeitenDiagnose Cure and Empower Yourself by Currents of Breath - Authored by Acharya Shriram SharmaGuiding Thoughts- Books by Pandit Shriram Sharma Acharya100% (19)
- F.1 - Respiratory Physio (For Quiz Muna)Dokument7 SeitenF.1 - Respiratory Physio (For Quiz Muna)Mac Vince HipolitoNoch keine Bewertungen
- 05 Goodacre 1994 Review Part 1Dokument8 Seiten05 Goodacre 1994 Review Part 1Ana Massiel NarváezNoch keine Bewertungen
- Utmb Usda ComplaintDokument9 SeitenUtmb Usda ComplaintHoustonPressNoch keine Bewertungen
- Uropati ObstruktifDokument22 SeitenUropati ObstruktifEvan Permana100% (1)
- Teaching Material On Camel Health and Production-By Theodros TekleDokument160 SeitenTeaching Material On Camel Health and Production-By Theodros TekleTheodros TekleNoch keine Bewertungen
- 3 QEBioDokument1 Seite3 QEBioSuperTotie LandritoNoch keine Bewertungen
- General Properties of VirusesDokument24 SeitenGeneral Properties of VirusesPeachy PieNoch keine Bewertungen
- Science Reviewer Grade 6Dokument2 SeitenScience Reviewer Grade 6Joy VinavilesNoch keine Bewertungen
- Shadow of The Demon Lord - Case of Consumption (Expert)Dokument6 SeitenShadow of The Demon Lord - Case of Consumption (Expert)KrallxNoch keine Bewertungen
- Review of HemodynamicsDokument99 SeitenReview of HemodynamicsAlessandro SilvaNoch keine Bewertungen
- Prevalence of Sarcoptic Mange in Rabbits: A. Meenakshisundaram and T. AnnaDokument6 SeitenPrevalence of Sarcoptic Mange in Rabbits: A. Meenakshisundaram and T. AnnaAchmad NugrohoNoch keine Bewertungen