Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Daftar Obat Puskes MerdekaDokument2 SeitenDaftar Obat Puskes MerdekaAnonymous aH8gCZ7zjNoch keine Bewertungen
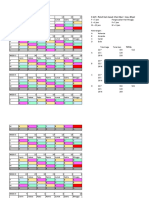
- 3 Shift: Pola 3 Hari Masuk 1 Hari Libur + Max. 40 Jam/mingguDokument4 Seiten3 Shift: Pola 3 Hari Masuk 1 Hari Libur + Max. 40 Jam/mingguAnonymous aH8gCZ7zjNoch keine Bewertungen
- Research Article: Characterization of Pediatric Acute Lymphoblastic Leukemia Survival Patterns by Age at DiagnosisDokument10 SeitenResearch Article: Characterization of Pediatric Acute Lymphoblastic Leukemia Survival Patterns by Age at DiagnosisAnonymous aH8gCZ7zjNoch keine Bewertungen
- ID Hubungan Faktor Resiko Dengan Terjadinya Nyeri Punggung Bawah Low Back Pain Pada PDFDokument10 SeitenID Hubungan Faktor Resiko Dengan Terjadinya Nyeri Punggung Bawah Low Back Pain Pada PDFAnonymous aH8gCZ7zjNoch keine Bewertungen
- Case HemoroidDokument19 SeitenCase HemoroidAnonymous aH8gCZ7zjNoch keine Bewertungen
- IT 3 - Spinal Cord InjuryDokument38 SeitenIT 3 - Spinal Cord InjuryAnonymous aH8gCZ7zjNoch keine Bewertungen
- Excercise 2 - Frequency MeasureDokument6 SeitenExcercise 2 - Frequency MeasureAnonymous aH8gCZ7zj75% (4)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Elements of Visual Design in The Landscape - 26.11.22Dokument15 SeitenElements of Visual Design in The Landscape - 26.11.22Delnard OnchwatiNoch keine Bewertungen
- ArticlesOfConfederation Constitution 3.0Dokument6 SeitenArticlesOfConfederation Constitution 3.0ChristinaNoch keine Bewertungen
- Thaligai Restaurant Menu 2021Dokument5 SeitenThaligai Restaurant Menu 2021harihar12Noch keine Bewertungen
- On Qbasic (Algorithm) : By: Nischit P.N. Pradhan Class: 10'B To: Prakash PradhanDokument6 SeitenOn Qbasic (Algorithm) : By: Nischit P.N. Pradhan Class: 10'B To: Prakash Pradhanapi-364271112Noch keine Bewertungen
- Chapter 5Dokument24 SeitenChapter 5Tadi SaiNoch keine Bewertungen
- Presentation On HR Department of Mobilink.Dokument18 SeitenPresentation On HR Department of Mobilink.Sadaf YaqoobNoch keine Bewertungen
- Breast Cancer ChemotherapyDokument7 SeitenBreast Cancer Chemotherapydini kusmaharaniNoch keine Bewertungen
- 01 History of Grammatical StudyDokument9 Seiten01 History of Grammatical StudyRomanNoch keine Bewertungen
- Detailed Lesson Plan in PED 12Dokument10 SeitenDetailed Lesson Plan in PED 12alcomfeloNoch keine Bewertungen
- Lesson Plan 2 Revised - Morgan LegrandDokument19 SeitenLesson Plan 2 Revised - Morgan Legrandapi-540805523Noch keine Bewertungen
- LITERATURE MATRIX PLAN LastimosaDokument2 SeitenLITERATURE MATRIX PLAN LastimosaJoebelle LastimosaNoch keine Bewertungen
- 3658 - Implement Load BalancingDokument6 Seiten3658 - Implement Load BalancingDavid Hung NguyenNoch keine Bewertungen
- The Peppers, Cracklings, and Knots of Wool Cookbook The Global Migration of African CuisineDokument486 SeitenThe Peppers, Cracklings, and Knots of Wool Cookbook The Global Migration of African Cuisinemikefcebu100% (1)
- Contract Law: Offer & Acceptance CasesDokument8 SeitenContract Law: Offer & Acceptance CasesAudrey JongNoch keine Bewertungen
- PPG ReviewerDokument8 SeitenPPG Reviewerryanbaldoria.immensity.ictNoch keine Bewertungen
- Fail Operational and PassiveDokument1 SeiteFail Operational and PassiverobsousNoch keine Bewertungen
- Gianna Pomata (Editor), Nancy G. Siraisi (Editor) - Historia - Empiricism and Erudition in Early Modern Europe (Transformations - Studies in The History of Science and Technology) (2006)Dokument493 SeitenGianna Pomata (Editor), Nancy G. Siraisi (Editor) - Historia - Empiricism and Erudition in Early Modern Europe (Transformations - Studies in The History of Science and Technology) (2006)Marcelo Rizzo100% (1)
- 150 Years of PharmacovigilanceDokument2 Seiten150 Years of PharmacovigilanceCarlos José Lacava Fernández100% (1)
- Thailand Day 2Dokument51 SeitenThailand Day 2Edsel BuletinNoch keine Bewertungen
- Software Quality Metrics MethodologyDokument17 SeitenSoftware Quality Metrics MethodologySumit RajputNoch keine Bewertungen
- Virtual Verde Release Plan Emails: Email 1Dokument4 SeitenVirtual Verde Release Plan Emails: Email 1Violet StarNoch keine Bewertungen
- Calcutta Bill - Abhimanyug@Dokument2 SeitenCalcutta Bill - Abhimanyug@abhimanyugirotraNoch keine Bewertungen
- Pemphigus Subtypes Clinical Features Diagnosis andDokument23 SeitenPemphigus Subtypes Clinical Features Diagnosis andAnonymous bdFllrgorzNoch keine Bewertungen
- NURS 406 Concept Map HyperparathyroidismDokument1 SeiteNURS 406 Concept Map HyperparathyroidismshyannNoch keine Bewertungen
- Sosa Ernest - Causation PDFDokument259 SeitenSosa Ernest - Causation PDFtri korne penal100% (1)
- Development Communication Theories MeansDokument13 SeitenDevelopment Communication Theories MeansKendra NodaloNoch keine Bewertungen
- Disorders of NewbornDokument4 SeitenDisorders of NewbornBRUELIN MELSHIA MNoch keine Bewertungen
- Lesson Plan in Science III ObservationDokument2 SeitenLesson Plan in Science III ObservationTrishaAnnSantiagoFidelNoch keine Bewertungen
- Ch3 Review QuestionsDokument15 SeitenCh3 Review Questionsave estillerNoch keine Bewertungen
- Network Scanning TechniquesDokument17 SeitenNetwork Scanning TechniquesjangdiniNoch keine Bewertungen